Chapter 7 Scalpels are the primary cutting instruments used to incise tissue (Fig. 7-1). Reusable scalpel handles (Nos. 3 and 4) with detachable blades are most commonly used in veterinary medicine; however, disposable handles and blades are available. Disposable scalpels with a locking retractable shield are designed to minimize the risk of surgical blade injuries while passing blades between procedural steps and during disposal (BD Bard-Parker, Franklin Lakes, NJ). Blades are available in various sizes and shapes, depending on the intended task. A No. 10 blade is most commonly used in small animal surgery for incision and excision of tissues. A No. 15 blade is a smaller version of a No. 10 and is used for precise incisions in smaller tissues. A No. 11 blade is ideal for stab incisions into fluid-filled structures or organs. The curved angle of the No. 12 blade limits its applicability, but it is most often used in cats for elective dissection onychectomy (declawing). FIG 7-1 Scalpel handles (left, No. 3; right, No. 4) and blades (top to bottom): Nos. 10, 11, 12, 15, and 20. Scalpels usually are used in a “slide cutting” fashion, which means that the direction of pressure applied to the knife blade is at a right angle to the direction of scalpel pressure. When incising skin, the scalpel blade should be kept perpendicular to the skin surface. Scalpels can be held with a pencil grip, a fingertip grip, or a palmed grip. The pencil grip allows shorter, finer, and more precise incisions than the other grips because the scalpel is at a 30- to 40-degree greater angle to the tissue (Fig. 7-2). However, this angle reduces cutting edge contact, making this grip less useful for long incisions. The fingertip grip offers the best accuracy and stability for long incisions. The palmed grip is the strongest hold on the scalpel and allows exertion of great pressure on the tissue, but this is often unnecessary in surgical situations. Scissors come in a variety of shapes, sizes, and weights and generally are classified according to the type of point (e.g., blunt-blunt, sharp-sharp, sharp-blunt), the blade shape (e.g., straight, curved), or the cutting edge (e.g., plain, serrated) (Fig. 7-3). Curved scissors offer greater maneuverability and visibility, whereas straight scissors provide the greatest mechanical advantage when cutting tough or thick tissue. Metzenbaum (also called Metz, Nelson, delicate, or tissue scissors) or Mayo scissors are most commonly used in small animal surgery. Metzenbaum scissors are more delicate than Mayo scissors and are designed for sharp and blunt dissection or incision of finer tissues; Mayo scissors are used for cutting dense, heavy tissue, such as fascia. Heavy scissors are used to cut suture, but these are separate instruments from those used to cut tissue. Suture scissors used in the operating room are different from suture removal scissors. The latter have a concavity on one blade to gently hook the suture away from the skin and facilitate easy removal. Delicate scissors (e.g., tenotomy scissors, iris scissors) are often used in ophthalmic procedures and other meticulous surgeries, such as perineal urethrostomy, that require fine, precise cuts. Bandage scissors have a blunt tip, which reduces the risk of cutting skin when the scissors are introduced under the bandage. Scissors should be utilized only for their specific purpose and should be regularly maintained to keep them sharp. FIG 7-3 Scissors. Left to right: stitch (suture removal), sharp-blunt, Metzenbaum, Mayo, wire, and tenotomy. Needle holders grasp and manipulate curved needles (Fig. 7-4). Size and type of needle holder are determined by characteristics of the needle to be held and location of tissue to be sutured. Larger needles require wider, heavier jawed needle holders. If needle holders are used to hold suture, the jaws should be finely serrated or smooth to prevent damaging the suture by fraying or cutting it. Long needle holders facilitate working in deep wounds. High-quality needle holders are made of noncorrosive, high-strength alloy and have a glare-free finish. The tips are hardened by coating them with a diamond surface or by fusing tungsten carbide to the face. Tungsten carbide inserts may be replaced when they become damaged or fail to hold suture adequately. Needle holders may be held using a palmed grip (no fingers are placed in the rings, and the upper ring rests against the ball of the thumb [Fig. 7-5]), a thenar grip (the upper ring rests on the ball of the thumb, and the ring finger is inserted through the lower ring [Fig. 7-6]), a thumb-ring finger grip (thumb is placed through the upper ring and the ring finger through the lower ring [Fig. 7-7]), or a pencil grip (index finger and thumb rest on the shafts of the needle holder [Fig. 7-8]), which is used with Castroviejo needle holders. The palmed grip is most advantageous for suturing tough tissue that requires a strong needle-driving force; however, the needle cannot be easily released and regrasped after a stitch without changing to another grip, making suturing less precise. Tissue (thumb) forceps are tweezer-like, nonlocking instruments used to grasp tissue (Fig. 7-9). The proximal ends are bonded together to allow the grasping ends to spring open or be squeezed shut. They are available in various shapes and sizes; tips (grasping ends) may be pointed, flat, round, smooth, or serrated with small or large teeth. Tissue forceps with large teeth should not be used to handle tissue that is easily traumatized. Tissue forceps with smooth tips, such as DeBakey forceps, are recommended for manipulation of delicate tissue, such as viscera or blood vessels. The most commonly used tissue forceps (i.e., Brown-Adson forceps) have small serrations on the tips that minimize trauma but facilitate holding tissue securely.
Surgical Instrumentation
Instrument Categories
Scalpels

Scissors

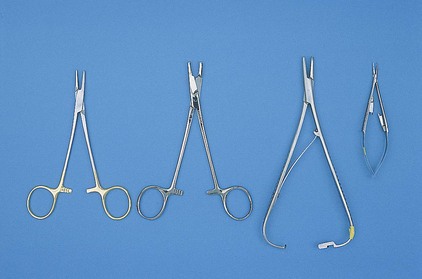
Needle Holders
Tissue Forceps
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Surgical Instrumentation