Chapter 93 Surgery of the Vagina and Vulva
The surgical procedures performed most commonly on the vagina and vulva are episiotomy, episioplasty, and excision of devitalized hyperplastic vaginal tissue. Episiotomy is performed to increase exposure for excision of vaginal or vestibular masses. Vaginal neoplasia is uncommon, and the majority of vaginal tumors are benign. Vaginal edema (previously referred to as vaginal hyperplasia) and vaginal prolapse occur only in intact females during estrus. Diseases of the external genitalia that require surgical intervention are rare in neutered females. See Chapter 92 for discussion of diseases of the vagina and vulva.
ANATOMY
Vagina
• The caudal boundary of the vagina is located cranial to the urethral opening, a point demarcated from the vestibule by a transverse mucosal ridge. A hymen normally is not present at the vestibulovaginal junction in the adult, although a vestige is retained in some females.
• The vagina is quite long in dogs, necessitating episiotomy for adequate surgical exposure. Caudal abdominal celiotomy may be necessary to gain surgical exposure to the cranial aspect of the vagina.
• The longitudinal folds (rugae) of the vaginal mucosa allow significant expansion in diameter during pregnancy and whelping.
• The dorsal median postcervical fold extends from the cervix and terminates caudally by blending with longitudinal folds of vaginal mucosa. This fold can be mistaken for the cervical os during vaginoscopy.
Vulva
The vulva (external genitalia) consists of three parts:
• The vestibule is the space between the vagina and the labia.
• The urethral tubercle (papilla), a ridgelike projection on the ventral floor of the vestibule caudal to the vestibulovaginal junction, contains the external urethral orifice.
• The clitoris is the homologue of the penis.
• The clitoris normally does not contain structures comparable to the os penis or the urethra of the male.
• The thinner constrictor vulvae muscle lies immediately caudal to the constrictor vestibule muscle.
EPISIOTOMY
Surgical Procedure
Technique
2. Position the dog in ventral recumbency, preferably in a perineal stand or an end of the surgical table that is elevated to raise the hindquarters.
7. Place surgical drapes so that the vulvar cleft and dorsal commissure are exposed. Exclude the anus from the surgical field.
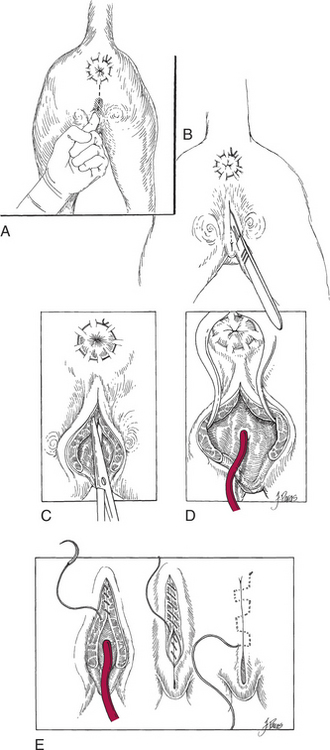
8. Insert a finger in the vestibule and identify the caudodorsal aspect of the vaginal canal. This point represents the dorsal extent of the episiotomy incision (Fig. 93-1A).
9. Make a median skin incision, beginning at the point described above and extending ventrally to include the dorsal commissure of the vulvar cleft (Fig. 93-1B).
10. Using Metzenbaum scissors, complete the episiotomy by incising the muscular layer and the mucosa in the same plane as the skin incision (Fig. 93-1C).
12. Close the incision in three layers (Fig. 93-1E).
a. Appose the mucosal edges with 3-0 absorbable suture material in a simple continuous pattern with knots exposed to the lumen.
b. Appose the muscular layer and subcutaneous tissue together with 3-0 absorbable suture material in a simple continuous pattern.