Chapter 160 Surgery of the Nasal Cavity and Sinuses
Signs in dogs and cats with chronic nasal and paranasal sinus disease may include nasal discharge, epistaxis, sneezing, gagging, stertorous breathing, nasal discomfort, and nasal deformity. Causes of nasal cavity and paranasal sinus diseases can be difficult to identify, but most cases are traumatic, infectious, inflammatory, mechanical, neoplastic, or parasitic in origin. Hemostatic abnormalities may lead to epistaxis. Most of these nasal diseases can be diagnosed and treated without surgery. However, rhinotomy may be necessary to arrive at a definitive diagnosis and may facilitate treatment of some diseases.
ANATOMY
Nasal Cavity
• The nasal cavity extends from the nostrils to the nasopharyngeal meatus and is divided into two chambers by the nasal septum. The rostral portion of the nasal septum is cartilaginous and difficult to evaluate radiographically.
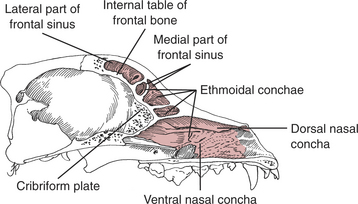
• The rostral nasal chambers are occupied by the dorsal and ventral nasal conchae (turbinates) (Fig. 160-1).
• The caudal nasal chamber is filled with ethmoidal conchae (turbinates). The ethmoidal conchae extend into the frontal sinus, forming narrow communicating ostia between the frontal sinus and the nasal cavity (see Fig. 160-1).
• In the cat, the nasal cavity is shorter, the ethmoidal conchae are larger, and the nasal conchae are smaller than in the dog.
• The cribriform plate is a sievelike partition between the nasal and the cranial cavities (see Fig. 160-1). It articulates with the frontal bones dorsally and the presphenoid bones ventrally and laterally.
• The blood supply to the nasal cavity originates from the external carotid arteries via branches of the maxillary artery, including the sphenopalatine, ethmoid, greater palatine, dorsal nasal, lateral nasal, and maxillary labial arteries.
Paranasal Sinuses
• The frontal sinus extends roughly from the medial canthus of the eyes to the temporal line. In dogs (but not in cats), it is divided into rostral, lateral, and medial compartments (see Fig. 160-1). The frontal sinus varies more in size than other cavities in the skull. The lateral compartment is particularly large in dolichocephalic breeds. Brachycephalic breeds have small lateral compartments, and the medial compartment may be absent.
• The maxillary sinus or recess is found dorsal to the roots of the third and fourth premolars and medial to the infraorbital canal. The maxillary recess in the cat is very narrow.
PREOPERATIVE CONSIDERATIONS
Disease Conditions
• Signs of chronic nasal disease can include unilateral or bilateral nasal discharge, epistaxis, sneezing, nasal discomfort, gagging, reverse sneezing, stertorous breathing, ocular discharge, and facial or nasopharyngeal distortion. Neurologic signs are seen if the disease extends into the cranium.
• The most frequent causes of chronic nasal and paranasal sinus disease are neoplasms, infections, and foreign bodies.
• Other causes include parasites (Pneumonyssoides caninum, Capillaria aerophila, Linguatula serrata), dental disease, trauma, lymphocytic-plasmacytic inflammation, and congenital anomalies. Nasal polyps, which are benign lesions, occur rarely.
Tumors
• Tumors of the nasal cavity and paranasal sinuses account for approximately 1% of all neoplasms in cats and dogs.
• Most intranasal tumors are diagnosed in older dogs and cats (>8–10 years) and in large-breed dogs.
• Most intranasal tumors are malignant (80%). Adenocarcinomas are most common, but squamous cell carcinoma, fibrosarcoma, chondrosarcoma, osteosarcoma, lymphosarcoma, hemangiosarcoma, undifferentiated sarcomas or carcinomas, and mast cell and transmissible venereal tumors also occur.
• The prognosis for malignant nasal neoplasms is guarded because of rapid local invasion and recurrence after therapy. Typically, these tumors do not metastasize until late in the course of the disease.
• Therapies that may help control some tumors include radiotherapy, immunotherapy, cryotherapy, and chemotherapy (see Chapter 26). These modalities are sometimes combined with surgical debulking of the lesion.
Infections
• Infections, especially those caused by fungal organisms, frequently cause nasal and paranasal cavity disease.
• Systemic diseases such as distemper, feline upper respiratory viral infections, and Rocky Mountain spotted fever can also cause acute or chronic rhinitis.
Fungal Rhinitis
• The most commonly reported pathogenic fungi are Aspergillus and Penicillium species in dogs and Cryptococcus neoformans in cats. Other reported pathogens are Rhinosporidium and Alternaria alternata.
• Patients with fungal rhinitis generally do not have facial distortion but may exhibit ulceration of the nares and more nasal discomfort than dogs with nasal neoplasia.
• Treatment of fungal rhinitis is primarily medical, although surgery may be necessary for definitive diagnosis or creating ports for medical therapy.
• Medical therapy may be systemic (itraconazole, ketoconazole, or thiabendazole), topical (enilconazole or clotrimazole administered directly into the nasal cavity), or both (see Chapter 163 for details).
• If indicated, perform topical therapy by placing fenestrated balloon catheters via endoscopy or rhinoscopy, placing indwelling fenestrated tubes into the frontal sinuses and nasal cavity, or creating a nasal stoma for nasal irrigation or swabbing.
Diagnosis
Physical Examination
• A small midline opening at the junction between the nasal planum and the skin suggests a nasal dermoid sinus cyst.
Diagnostic Imaging
Radiography
• Include lateral, ventrodorsal, rostrocaudal, and rostroventral-caudodorsal open-mouth or occlusal radiographic views (see Chapter 4).
• The two most useful radiographic views are the ventrodorsal view of the maxilla using intraoral radiographic film and the rostrocaudal projection highlighting the frontal sinuses.
Rhinoscopy
• The rostral aspect of the nasal cavity may be seen with an otoscope, cystoscope, or small fiberoptic scope. A flexible pediatric bronchoscope or 2- to 3-mm diameter rigid telescope facilitates examination of the remainder of the cavity and allows retropharyngeal examination of the choanae for lodged foreign bodies, nasal mites, mucosal invasion (mycoses), or extruding nasal tumors.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


