Chapter 60 Surgery of the External Ear Canal and Pinna
External ear canal surgery is performed to provide exposure and drainage for the vertical and horizontal ear canal or to remove irreversibly infected tissue or neoplasia. Procedures for the external ear canal include lateral ear canal resection, vertical ear canal ablation, and total ear canal ablation. Drainage of auricular hematoma is the most common surgical procedure of the pinna; this is discussed later in this chapter.
Success of ear surgery relies on the following:
GENERAL SURGICAL INDICATIONS
External ear surgery rarely is indicated in the cat except for traumatic or neoplastic conditions. Inflammatory polyps extending into the external ear canal from the tympanic cavity usually do not require external ear surgery for removal. See middle ear surgery (see Chapter 62) for further information.
ANATOMY
External Ear Canal
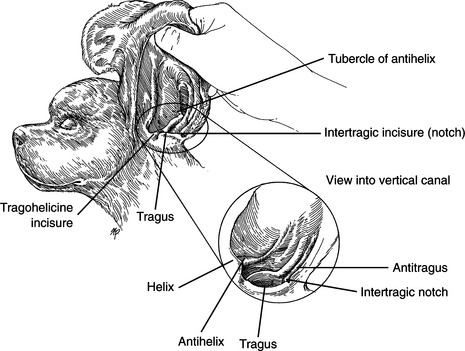
Important Local Structures
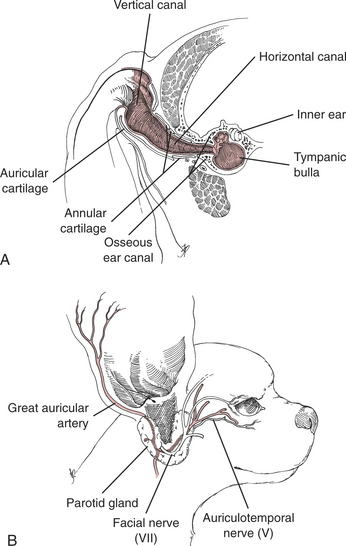
Blood Vessels (Fig. 60-2B)
Nerves (Fig. 60-2B)
PREOPERATIVE CONSIDERATIONS
An accurate preoperative diagnosis along with determination of the extent and severity of disease is important when choosing the surgical procedure. Attempt to identify and control any systemic skin condition before surgery. Changes in the ear canal that usually represent irreversible disease include neoplasia, thickening and calcification of cartilage, and firm hyperplastic or proliferative epithelium. Determine if middle ear disease is present concurrently since exploration and drainage of the middle ear is recommended in addition to surgical treatment of the external ear disease (see Chapter 62).
Ear Palpation
Neurologic Examination
Radiographic Examination
Otoscopic Examination
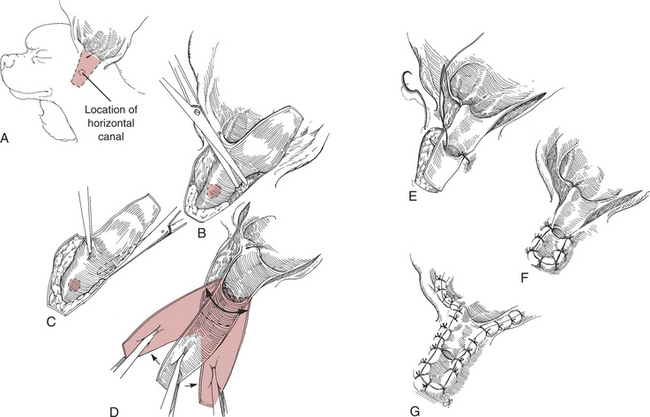
LATERAL EAR CANAL RESECTION—ZEPPS MODIFICATION (LECR)
Surgical Procedure
Objectives
Technique (Fig. 60-3)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


