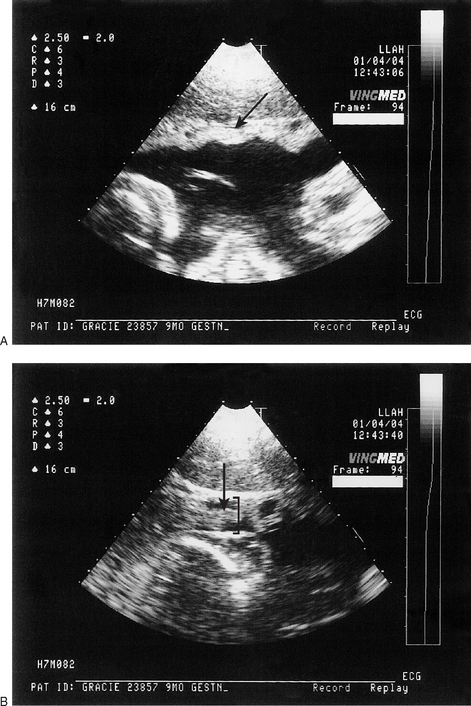
Chapter 2 Perinatal death accounts for a significant proportion of foal mortality and a significant number of deaths occur during what may appear otherwise to be a normal pregnancy. Noteworthy advances have been made in the achievement of pregnancy and considerable interest has been focused on parturition and the early adaptive period of the foal. Although these events are clearly vital, they actually occupy a trivial proportion of the total gestational length. There is considerable scope for problems during the time that up to now has been largely ignored. Only recently has any significant interest been focused on the gestational development of the foal. With the improved success in fertility and in treating sick neonates, the importance of fetal assessment has also increased and there is now an increasing awareness of the potential benefits in monitoring fetal health. Prepartum abnormalities in the mare are relatively common and cause considerable concern amongst owners; this is justifiable because of the intimate dependence of the foal upon the mare. The placental unit provides a barrier between the circulation of the mare and that of the foal and the foal relies totally on this. Disease processes and developmental abnormalities may affect the equine fetus in much the same way as the neonate and adult horse. However, because of its hidden location it is difficult to examine the developing foal completely and to assess its well-being. These limitations also severely limit the therapeutic options. Information gained during antepartum assessment is important for the management of both the mare in late pregnancy and the newborn foal. Information gleaned from regular fetal and maternal clinical assessments provides essential information for the attending staff. • Vulval/vaginal discharge (Fig. 2.1): this can be a very important clinical sign. The origin of the discharge should be established by careful vaginoscopic examination. Where a purulent discharge originates from the external cervical os a detailed ultrasonographic examination is always required. This may identify a focal (centered around the cervical star) or diffuse placentitis. The foal will be threatened by either state. Even a generalized vaginitis can be a serious problem with a major risk of ascending infection. • Premature mammary development and premature lactation: this is an important sign that may indicate the presence of placentitis or twins. A detailed clinical and ultrasonographic investigation is indicated. • Maternal colic: maternal intestinal colic is common in pregnant mares but colic signs may be indistinguishable from those caused by uterine torsion or retroflexion. Impending abortion often causes abdominal pain. This possibility must be considered in all pregnant mares presented for colic investigation. • Maternal malnutrition and concurrent disease: the nutritional and concurrent health status of the mare will have an inevitable consequence on the well-being of the foal. However, in spite of severe malnutrition it is remarkable how bright a foal can be at birth. Even if the foal is in poor physical condition at birth it can still survive if the mare has a strong maternal instinct and reasonable milk supply. Where the mare has concurrent illness the threat to the foal may be much greater. In some cases total intervention has to be provided if the foal is to have any chance of survival. • Prolonged gestation: there is a wide variation in the gestational length in mares but inordinately prolonged gestation is a serious event that warrants careful investigation. In some cases this is simply a matter of embryonic diapause where development of the fetus is delayed. The outcome in the latter case may be completely satisfactory and this can be predicted to some extent if a regular thorough fetal and maternal assessment is made. In some cases, however, the prolongation may be due to fetal mummification. The maintenance and termination of pregnancy are not controlled by ovarian activity after 45 days and so, without regular assessment, there may be no indication of an abnormality. • Prior history of twins, abortion, stillbirth, prematurity, or dysmaturity: the mare’s breeding history may be a significant reason for fetal assessment. Recognition of abnormal fetal development or placental thickness, etc. can be identified and, even though the therapeutic options are limited, extra care can be given to minimize further risks. A full fetal assessment protocol would be as follows: • pawing the ground, looking round at flanks • cringing of the hindquarters and clamping of the tail. • occasionally a mare may rub her hindquarters against a wall. • curling of the upper lip in the Flehmen posture is common. Udder development and distention of teats • Mammary growth begins about a month before parturition but the major increment in udder size occurs in the last 2 weeks. The teats become shorter and fatter as the udder becomes full because the bases of the teats are stretched. However, as the time for delivery becomes imminent, the teats fill with milk, elongate and become more tender to the touch. The presence of edema of the udder and ventral body wall are additional indications. • White flecks are often seen on the teats themselves a few days before the mare ‘waxes up’. Many mares ‘wax up’ 24 hours before birth, a term given to the clotting of a bead of colostrum at the end of the teat (Fig. 2.2). The lack of wax is not indicative that parturition is a long time off, because these plugs may be dislodged, especially in active mares turned out. Similarly, most mares that prematurely deliver or abort will not “wax-up”. These changes occur to allow passage of the foal during delivery. • Relaxation of pelvic ligaments (i.e. sacroiliac and sacrosciatic) and softening either side of tail head several days before parturition. A ‘hollowness’ may start to appear either side of the tail head and, if the area either side of the tail head is felt daily in the last 3 to 4 weeks of pregnancy, it may be possible to detect this change as the muscle tone relaxes. • Relaxation and lengthening of the vulva several days before birth. • Relaxation and softening of the cervix shortly before birth. Transrectal ultrasonography (see also p. 379) • In early gestation, transrectal imaging has revolutionized the detection of pregnancy, identification of multiple conceptions, and determination of fetal sex. • Throughout pregnancy it allows examination of the placenta, although from mid to late gestation only the cervical pole can be visualized fully. Therefore, detection of ascending placentitis is possible. There are published values for expected placental thickness, etc., throughout the last trimester.2 • The normal combined thickness of the uterus and placenta (CTUP) at the ventral aspect of the uterine body and near the cervical–placental junction is reported to be < 7 mm before 300 days’ gestation. • Mares at risk of placental failure have CTUPs > 8 mm at 271–300 days and > 10 mm at 301–330 days. Transabdominal ultrasonography • Ultrasonography is now used routinely to evaluate the equine fetus.3,4 The fetal thorax is usually the most easily identified structure; the fetal heart can be readily identified contracting in the cranial thorax with the major blood vessels passing caudally, the aorta lying next to the spinal vertebrae. The diaphragm can be recognized separating the thoracic and abdominal cavities and fetal breathing movements may be noted. In the fetal abdomen, the fluid-filled (anechoic) stomach, kidneys and liver are all easily identified. • In mid and late gestation it allows maximal visualization of the pregnancy (placenta, fetal fluids and fetus), enabling assessment of fetal health and development. • The ultrasound scanners used for routine broodmare examinations are suitable for fetal imaging; however a 3.0 or 3.5 MHz probe is ideally needed because of its extra penetration. Linear array transducers give the widest field of view with an easily interpretable image, although sector transducers can also be used. Good mare preparation will improve image quality and reduce artifacts. • The mare’s ventral abdomen should be free of dirt and closely clipped with a fine blade from the sternum to the udder either side of the midline. • Removal of all grease in the skin by using a soapy wash and a spirit final wipe. • Generous application of high viscosity ultrasonic coupling gel is important. • The probe is orientated longitudinally, approximately over the mare’s midline and then the fetus is located by scanning from side to side. • Careful evaluation of the placenta is best performed with a 5 or 7.5 MHz transducer. The average combined uteroplacental thickness in late gestation is 1.15–1.26 ± 0.33 cm.3,4 • A mare with a placental thickness of greater than 2 cm is likely to be suffering from placentitis (Fig. 2.6). Figure 2.6 A transabdominal ultrasound scan of a pregnant Irish-cross mare at 310 days gestation showing (A) a normal area of placentation and (B) an area showing marked placentitis as indicated by placental thickness (bracket) and separation (arrow). • Both the allantoic and amniotic fluid compartments can be imaged. In normal pregnancies of more than 300 days the mean depth of allantoic fluid is 13.4–19 ± 4.4 cm.3,4 The maximal depth of amniotic fluid is 7.9 ± 3.5 cm. Normal amniotic fluid is always ultrasonographically clearer than normal allantoic fluid. Amniotic fluid has significantly fewer echogenic particles;4 hyperechoic particles in the amniotic cavity may be associated with the presence of meconium. A single or few larger hyperechoic particles (hippomanae) can be observed in allantoic fluid as early as 36 days prepartum and in all mares at 10 days prepartum. Excessive amounts may indicate the presence of abnormal quantities of blood. • Using ultrasound guidance it is possible to collect amniotic and allantoic fluid samples although the technique carries relatively high risks of premature delivery and abortion.5,6 The ratio of lecithin to sphingomyelin in amniotic fluid has been shown to be important in indicating pulmonary maturity in the human but this has not yet been shown to be the case in horses and so the clinical value of the procedure is not yet established.7 • Exercise of the fetus is probably a necessary function for proper neuromuscular and anatomical development. Fetal activity is greatest between 3 and 4 months’ gestation. During a routine scan of 20–30 minutes’ duration it is unusual to see periods of more than a few minutes of fetal inactivity or sleep. • Fetal activity is probably suppressed in later gestation and, while activity can be induced and does occur spontaneously, there may be a general impression of a significant reduction in observable fetal movement. Fetal limb movements can be seen in the mare’s lower flank area, especially when close to foaling. • Considerable reflex activity increases within 3 days of foaling enabling the foal to attain the correct presentation, position and posture for delivery. 4. Fetal position changes (Fig. 2.7): • Three terms are usually used to describe the way in which the fetus lies in the uterus. These are: • In the first 5 months of gestation, the fetus spends an equal amount of time in anterior and posterior presentation, but is usually ventral (and often slightly laterally) with the limbs flexed. In about the sixth month of pregnancy, the fetus assumes an anterior presentation, ventral position and flexed posture. After 7 months, more than 90% are in anterior presentation and, by term, less than 1% are in posterior presentation. • During first stage labour, the fetus extends its head and forelimbs. This is followed by rotation into the dorsal position. This repositioning process may be assisted by myometrial contractions, the influence of the mare getting up and down and changing from recumbency on one side to the other and rolling. This fetal turning is usually complete by the time the fetus enters the birth canal ready for delivery (second stage labour). • Fetal heart rate and rhythm can be determined by ultrasound examinations (Fig. 2.8). Measurements can be made directly by counting the number of fetal heartbeats over a defined period of time; alternatively, the ventricular contraction interval (R–R) can be derived from M-mode ultrasound. The most useful analysis is made from continuous measurements of heart rate, recorded over periods of 10 minutes or more, and relating this to fetal activity. Some specialists prefer Doppler heart rate monitors or fetal electrocardiograms for this assessment. • The mean fetal heart rate falls with increasing gestational age from 120 beats per minute at 160 days gestation to 76 ± 8 beats per minute in the last 30–50 days (Fig. 2.9). This drop is probably the result of naturally increasing parasympathetic tone in the developing fetus. Figure 2.9 Graph showing fetal heart rate throughout gestation with key points at 160 days (heart rate approx 120 b.p.m.) and at 340 days (heart rate approximately 80 b.p.m.). The figures apply to data derived from ponies but there may be some breed variations. • In general, signs of fetal distress include: • Simple observation in relation to spontaneous fetal movements is known as the non-stress test. The following normal reactive pattern has been reported:3 • There are also stress tests in which induced oxytocin contraction and acoustic stimulation are used as stimuli for fetal activity.8 The umbilical cord can be seen floating within the fetal fluids. The two arteries, one vein and urachus are identifiable ultrasonographically (Fig. 2.10). Blood flow measurements through the umbilical arteries and vein can be made using Doppler flow (Fig. 2.11). Measurements of specific bone lengths and diameters are difficult to measure consistently in equine fetuses and therefore the aortic and vena cava diameter and the diameter of the orbit (Fig. 2.12) are used. The aorta is the easiest to routinely find and measure (Fig. 2.13). Figure 2.13 Graph showing the equine fetal aortic diameter in Thoroughbred foals. There may be some breed variations. • The great vessels are measured in a longitudinal plane using the scanner’s electronic callipers. • The aorta is measured with the frame frozen in systole at the level of the caudal border of the heart. • In the Thoroughbred fetal aortic diameter ranges from 21–22.8 ± 2.1 mm at 300 days to 27 mm at term.4 • This correlates significantly with foal weight at birth and therefore provides an effective measurement of fetal growth. • Measurements have been incorporated in the following equation: Estimated fetal weight = −19.62 + (29.25 × Ao diameter in mm). • Using this technique estimates of fetal weight are within 3.5 kg. • This can be used to predict the small fetus in a high risk pregnancy. Factors that may be associated with a ‘small-for-dates’ fetus or a growth-retarded fetus include: • Twin pregnancy in the mare is generally (and justifiably) viewed as a potential disaster. Early recognition is critical and ultrasonography has revolutionized their detection. Twins can be detected from 10 days after conception by transrectal ultrasound. A hyperechoic structure may be noted separating the twins; this is probably a reflection of the avillous placental contact area (see p. 54). From approximately 90–100 days’ gestation transabdominal ultrasound for assessment of twins is possible (Fig. 2.14). • Fetal reduction is a standard technique in equine stud farm medicine and this is described in standard reproduction texts. It is critical that fetal reduction should take place within 14–21 days of conception and this is a major use of early ultrasonographic examination. Twin pregnancies over 45 days of age can be much more difficult to ablate and ultrasonographic guidance can be used to support twin reduction by: A single abnormal ultrasonographic measurement is not always accurate in indicating the probability of a poor fetal outcome. For this reason a combination of variables can be used to identify the potential ‘at risk’ fetus.12 Two points are allocated to each of the following parameters (2 points if normal and 0 points if abnormal): Straightforward ultrasound examination without biophysical profiling is less efficient at predicting the outcome of the pregnancy but this assessment is also influenced by events at delivery. The value of ultrasonographic assessments, involving either biophysical profiling or simple subjective evaluation, is probably therefore best for abnormal pregnancies; a normal assessment should probably not be taken to suggest that the pregnancy will terminate normally. There are far too many subsequent variables to predict normality. Nevertheless there are still some cases in which the negative findings do not correlate with a subsequently normal foal.13 Figure 2.15 Fetal ECG trace showing the faint recordings of the fetal activity (F) with the more obvious maternal activity (M). The fetal rate is approximately 130 b.p.m. while the maternal rate is approximately 40 b.p.m. • This has been used for many years as an index of fetal viability and normality but the technique still lacks sensitivity. It is applicable only after 150 days of gestation and it can provide information about fetal positioning and viability and may detect twinning. The procedure is easy to perform using standard electrocardiographic equipment and is non-invasive. It is possible to make continuous recordings of heart rate and so detect changes that may not be identified during shorter-term ultrasonography. • In normal pregnancies the fetal heart rate falls from around 120–130 before day 160 to 60–70 in the last month of gestation. The fetal heart is normally free of arrythmias. A transient increase in fetal heart rate may be detected between 220 and 290 days, which probably corresponds to a period of increased fetal activity. • Prepartum arrythmias and prolonged alterations in heart rate are associated with fetal abnormality and abnormal pregnancies.14 These are useful for assessing the general health status of the mare, inflammatory profile, etc. • Two estrogen groups can be measured in the pregnant mare. • Estrogens are measured in mid gestation, from 120 to 280 days, reaching a peak at 210 days. • The fetal gonads produce equilin and equilenin and so their presence confirms the existence of a live fetus.15 Figure 2.16 The endocrinology of late pregnancy. Estrogen production begins to fall just before parturition (arrow). Pregnanes slowly reduce over the last 4 weeks of pregnancy and decrease precipitously immediately at parturition. Progesterone gradually increases during the last month of gestation and then falls rapidly after foaling. Prostaglandin is significantly increased during stage 1 of labor with peak concentrations achieved during stage 2. Oxytocin peaks during stage 2 of labor immediately following the prostaglandin surge. Prolactin gradually increases over the last month of pregnancy, peaks at around 30–60 days after parturition and then tapers off over the next 2–4 months. • Progesterone is produced by primary and secondary corpora lutea in the ovary, but the placenta takes over the role during the first 3 months of pregnancy and ultimately becomes the only source of progesterone. The corpora lutea become irrelevant by 150 days.16 The developing fetus and placenta produce other progestagens from around day 60 that support the pregnancy. • These are measured in late gestation. • Concentrations in the normal mare rise during the last month of pregnancy and then fall dramatically during the last 2 to 3 days. The late gestation surge in progestagens is possibly induced by increased fetal adrenocortical activity. Precocious rises in these hormones may be associated with placental pathology. • Abnormally low progestagens are reported in mares with non-viable or dead fetuses associated with equine herpesvirus infection (see p. 280). • Before 300 days, placental dysfunction/problems may be diagnosed from early plasma progestagen increases. • This is a specific glycoprotein derived from the fetal liver that is used in other species to provide information on fetal status. Normally the protein is retained in the fetal circulation with only minute amounts crossing the placenta. • Death of the fetus (with massive release into the placental tissues and amniotic fluid) or increased permeability of the placenta, result in significantly increased concentrations in the maternal circulation. • It is elevated in late pregnancy mares in which there are twinning, placentitis, premature placental separation, uterine trauma and fetal death.17
RISK CATEGORY OF THE FOAL
ASSESSMENT OF FETAL HEALTH AND PREPARATION FOR BIRTH
PREPARTUM ABNORMALITIES IN THE MARE
MONITORING FETAL HEALTH DURING GESTATION
Mare’s history
Physical examination
Signs of impending abortion, premature delivery or parturition
Behavioral changes
Mammary changes
 Typically mammary secretions change from straw-colored water-like secretions becoming cloudier in the weeks preceding parturition, ending up as white-yellowish and viscous (colostrum) close to delivery (Fig. 2.3).
Typically mammary secretions change from straw-colored water-like secretions becoming cloudier in the weeks preceding parturition, ending up as white-yellowish and viscous (colostrum) close to delivery (Fig. 2.3).
 It can be normal for mares to ‘run milk’ (Fig. 2.4) for hours, days or even weeks before parturition.
It can be normal for mares to ‘run milk’ (Fig. 2.4) for hours, days or even weeks before parturition.
 If a mare runs milk it may be a good idea to milk her out and collect and store the colostrum.
If a mare runs milk it may be a good idea to milk her out and collect and store the colostrum.
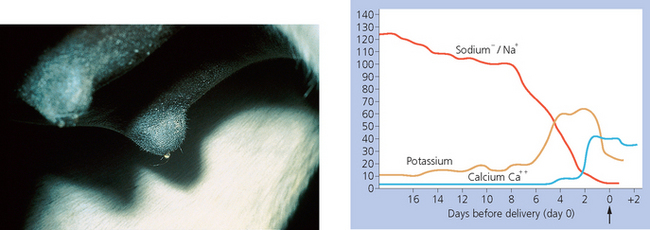
 Changes in electrolyte composition of mammary secretions during late pregnancy (Fig. 2.5) have been used to determine fetal readiness for birth.1
Changes in electrolyte composition of mammary secretions during late pregnancy (Fig. 2.5) have been used to determine fetal readiness for birth.1
 Immediate prefoaling changes are an increase in calcium (> 10 mmol/L) and potassium (> 35 mmol/L), and a decrease in sodium (< 30 mmol/L).
Immediate prefoaling changes are an increase in calcium (> 10 mmol/L) and potassium (> 35 mmol/L), and a decrease in sodium (< 30 mmol/L).
 Field test kits are available.
Field test kits are available.
Perineal changes
Fetal imaging
 Presentation refers to the region of the fetal body presented to the pelvic inlet (e.g. anterior means ‘head first’).
Presentation refers to the region of the fetal body presented to the pelvic inlet (e.g. anterior means ‘head first’).
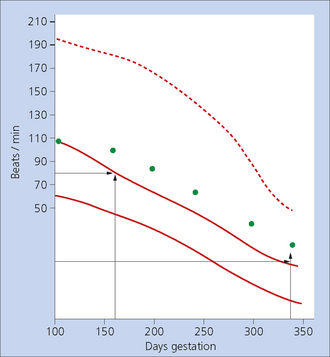
 sustained tachycardia without fetal activity: heart rates of over 200 beats per minute in the 120–220 day period or over 110 beats per minute in the last 2 months signify possible fetal distress
sustained tachycardia without fetal activity: heart rates of over 200 beats per minute in the 120–220 day period or over 110 beats per minute in the last 2 months signify possible fetal distress
 bradycardia: heart rates less than 60 beats per minute indicate fetal distress or depression.
bradycardia: heart rates less than 60 beats per minute indicate fetal distress or depression.
 an average of 10 accelerations in a 10-minute period
an average of 10 accelerations in a 10-minute period
 baseline heart rate of 60–92 beats per minute
baseline heart rate of 60–92 beats per minute
 baseline variability (i.e. normal fluctuations) of 7–15 beats per minute
baseline variability (i.e. normal fluctuations) of 7–15 beats per minute
 accelerations: amplitude 25–40 beats per minute
accelerations: amplitude 25–40 beats per minute
 duration of periods of normal increase around 23–36 seconds.
duration of periods of normal increase around 23–36 seconds.
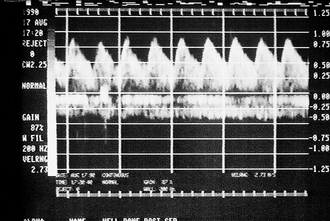
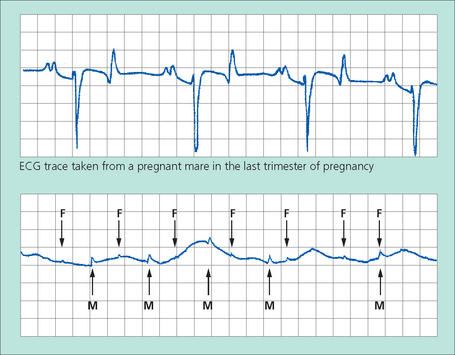
Fetal electrocardiography (Fig. 2.15) (see p. 381)
Blood samples
Hematology, biochemistry
Endocrinology
Estrogens
 Estrone sulfate: this requires both the fetus and the placenta for its synthesis and concentrations can reflect fetal viability and fetoplacental status
Estrone sulfate: this requires both the fetus and the placenta for its synthesis and concentrations can reflect fetal viability and fetoplacental status
 β-unsaturated estrogens (equilin and equilenin): these are unique to the horse.
β-unsaturated estrogens (equilin and equilenin): these are unique to the horse.
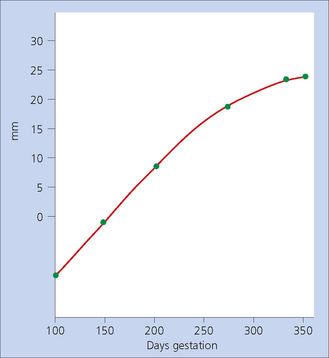
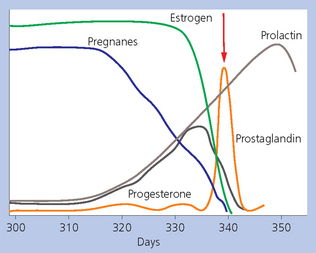
Progestagens (Fig. 2.16)
Alpha fetoprotein (AFP)
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree