CHAPTER 96 Reproductive Surgery in the Boar
Current swine breeding management strategies have placed an increased emphasis on the clinician’s technical proficiency in performing boar reproductive surgery. Use of surgically sterilized boars in gilt development and institution of estrus detection programs have become commonplace in many of today’s production systems. Critical, scrutinized genetic selection and the preferred distribution of these desired genetic traits through artificial insemination also have placed increased value on the boars that are standing at stud. It is not uncommon for boars selected for artificial insemination programs to have values 25 to 50 or more times greater than their market hog counterparts. These many varied factors contribute to the necessity for a clinician to be able to provide attention to the individual boar’s health and reproductive viability and function.
GENERAL ANESTHESIA
Most surgical procedures performed in adult boars require the use of general anesthesia.1–3 Drug combinations that have been used successfully to provide 30 to 60 minutes of general anesthesia include the following: (1) xylazine hydrochloride (2 mg/kg of body weight) plus tiletamine hydrochloride–zolazepam hydrochloride (Telazol*) (6 mg/kg), administered intramuscularly [IM]; (2) xylazine (1 mg/kg) plus butorphanol tartrate (0.1 mg/kg) plus Telazol (3 mg/kg), administered IM; (3) Telazol (5-ml vial) reconstituted with 2.5 ml of xylazine (100 mg/ml) and 2.5 ml of ketamine (100 mg/ml), with the resulting mixture given IM at a rate of 0.02 to 0.04 ml/kg; or (4) premedication with xylazine (2 mg/kg given IM), followed in 10 minutes with intravenous administration of a 5% solution of thiopental sodium, given to effect. Animals should be isolated from herdmates during the recovery period. With any of the surgical techniques outlined, it is preferable to keep recovered boars isolated from other swine for at least 10 to 14 days after surgery to allow healing. Exposed skin sutures should be removed before reintroduction to herdmates, because pigs are curious animals and frequently will pull or bite on the sutures.
CORRECTION OF PERSISTENT PENILE FRENULUM
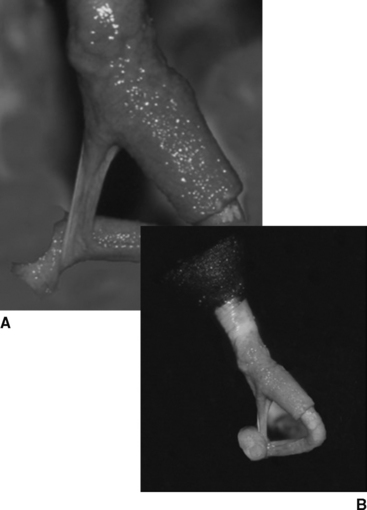
The frenulum is an epithelial attachment that runs from the mucosal covering of the penis to the base of the corkscrew behind the tip of the penis. This tissue normally is present in prepubertal and peripubertal boars, with breakdown and detachment occurring as a normal event in boars at or just before puberty. With failure of this breakdown process, the penis will “fishhook,” or turn backward, when penile extension occurs (Fig. 96-1). Boars with persistent penile frenulum cannot successfully initiate coitus but sometimes can have their semen collected using the gloved hand technique. Depending on severity, surgical correction of this condition can be performed either during semen collection or with the animal under general anesthesia. Resection or, better yet, removal of this tissue is most easily accomplished using scissors. Hemorrhage is minimal, negating the need for ligation before or after excision. The animal can be used for breeding 10 to 14 days after surgery. Because persistent penile frenulum is thought to be heritable, breeding stock should not be selected from the offspring sired by affected boars.
REPAIR OF PREPUTIAL PROLAPSE
Prolapse of the prepuce in the boar is uncommon. In such an occurrence, however, quick action is paramount to successful replacement of viable tissue and minimization of edema. With the animal under general anesthesia, prolapsed tissue should be manually replaced. After replacement, a purse-string suture, using a 1 nonabsorbable monofilament suture, is placed around the preputial orifice. The purse-string suture should be tightened sufficiently to retain prolapsed tissue yet be loose enough to maintain patency for urination. Flushing of the preputial cavity with a warm, antiseptic solution is often performed daily over a 3- to 5-day period after replacement. At the end of treatment, the purse-string suture is removed, and the boar returned to service after an additional 14 days of sexual rest.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


