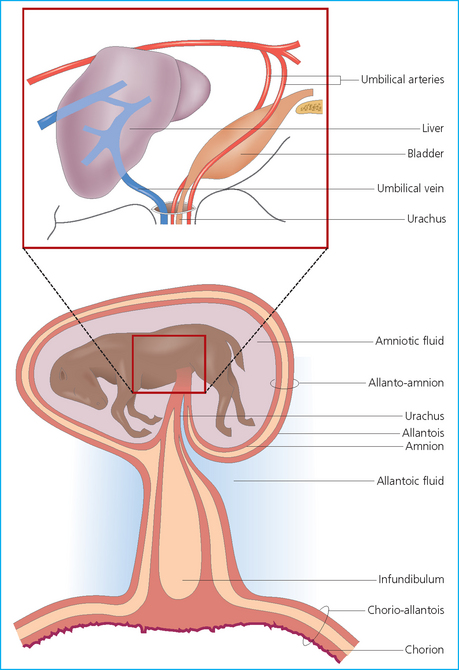
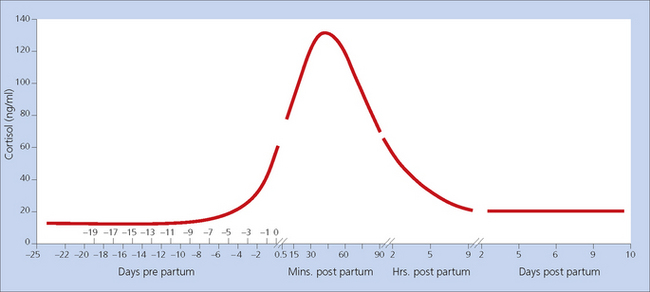
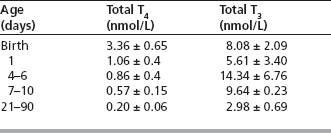
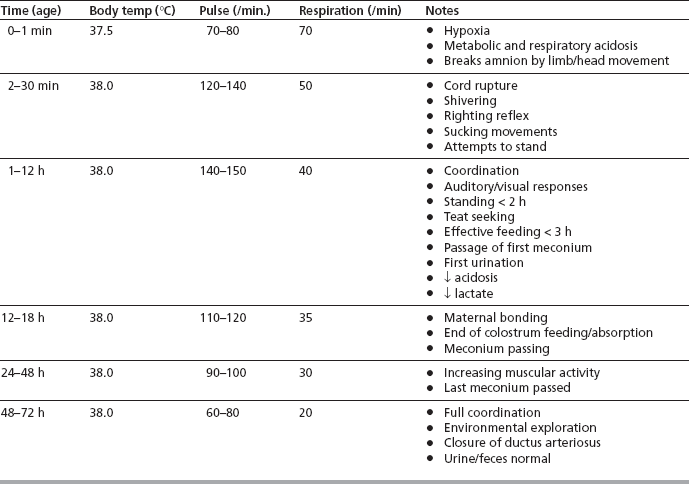
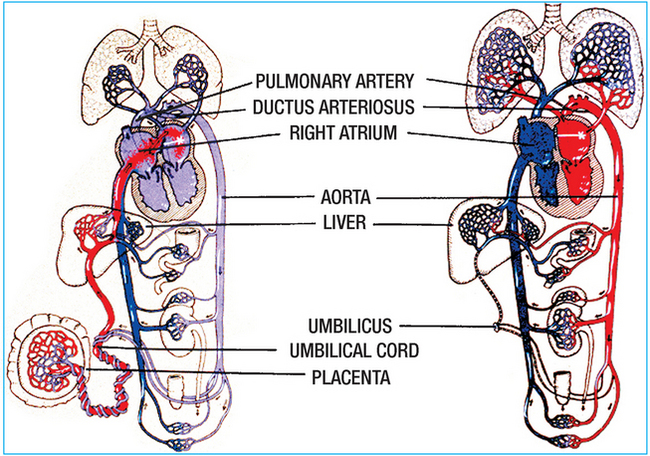
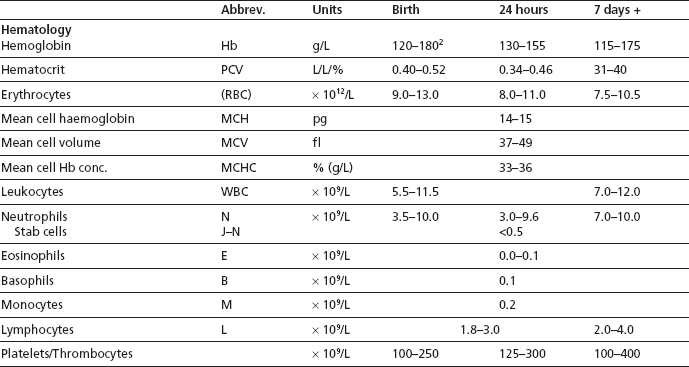
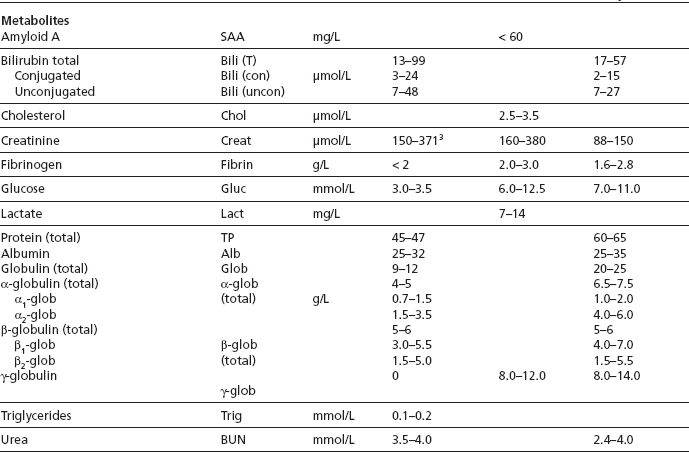
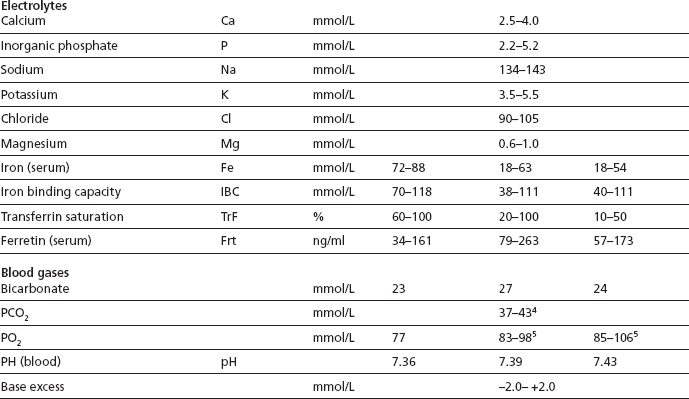
Chapter 1 Passage of the foal through the birth canal provides significant beneficial thoracic compression that serves to drive excess fluid from the airway. Foals delivered by cesarean section do not have this mechanism and so need to have extra care to establish a clear airway (see p. 71). At the moment of birth the lungs must expand and the pulmonary circulation must be ‘switched on’ to ensure a perfect ventilation perfusion match between the two sides of the circulatory system (Fig. 1.1). The change to pulmonary breathing and the circulatory adjustments that must accompany such a change within minutes of birth must be perfect if the foal is to survive and be able to move quickly to ensure safety.1 Up to this point the blood from the pulmonary artery is shunted via the ductus arteriosus into the aortic circulation as a result of the high resistance afforded by the collapsed lungs and the relatively low aortic pressure. Oxygen-saturated blood arriving in the caudal vena cava from the placental vessels passes through the foramen ovale to the left atrium so that the brain receives freshly oxygenated blood. This is obliterated within the first few weeks of life.2 Figure 1.1 Theoretical diagram of the fetal and adult circulations. (*Foramen ovale: open in fetus, closed in neonate) The adaptations that result in a change from a fetal to an adult circulation require a transition stage during which various parts of the cardiorespiratory system undergo significant changes. There may be some variations during this time as these adaptations take place and mature. Within minutes of birth the foal’s heart rate may normally be as low as 50–60 beats per minute but this rapidly increases to over 120 beats per minute. Arrhythmia, including atrial fibrillation, atrial tachycardia and extraventricular depolarization, is also common in newborn foals within the first 15–30 minutes of life. However, although these could be alarming they are almost invariably due to high vagal tone and will resolve spontaneously over a short period.3 It may be unwise to perform an electrocardiographic examination on a very new foal because the results may be misleadingly and possibly alarming! The differentiation of the abnormal foal from the normal one can be difficult and may be a significant clinical challenge. The highly elastic nature of the ductus arteriosus means that some shunting one way or the other is present for up to 48–72 hours, but thereafter it closes and becomes a fibrous band.4 The ductus arteriosus undergoes significant preparatory changes in utero several days prior to birth in the normal situation.5 In induced parturition, cesarean section or premature birth these preparatory events may not have occurred and the foal will be a risk for a patent ductus arteriosus. Therefore, failure of the ductus arteriosus to close in the first few days of life is a recognized pathological entity and is recognized as a typical machinery-like murmur with maximal audible sounds over the upper (base) regions of the heart (this condition is described in detail on p. 115). Failure of the foramen ovale to close is extremely rare in horses and is probably detected and confirmed only by detailed ultrasonographic examination. By far the commoner abnormality that is audible at birth is a defect in the interventricular septum and here a typical systolic murmur with maximal intensity on the right side is heard (see p. 117). Foals born dead that have never made any effort to expand the lungs will have almost solid lungs when examined at necropsy; a sample of the lung tissue will not float in water. It is possible also that the foal may have died after insufflation of the lungs, in which case the lungs will be found to be expanded (to a varying extent) and will float in water. Failure to expand a portion of the lungs at birth is a recognized pathological condition (fetal atelectasis) and is described on page 275. The thorax of the newborn foal is very compliant and so it must make active respiratory movements for both inspiration and expiration. This has implications for restraint and it is possible to impair breathing simply by having to restrain the foal. The minute volume of the foal is more than double that for the adult horse and this is probably because of the need to move air through a higher dead-space volume and to cope with the high metabolic rate of the newborn. Also the chest wall of the newborn foal is very compliant and so any respiratory disorder may have a disproportionately adverse influence on lung efficiency.6 The position the foal adopts also influences the oxygenation of blood. A foal in lateral recumbency will probably have a markedly lower partial pressure of arterial oxygen than one in sternal recumbency (Fig. 1.2). This forms one of the most important principles of the management of neonatal foals. • Surfactant is a complex of phospholipids, which is produced (and stored) in specialized alveolar cells. It has very potent effects on surface tension. This and the other functions of the lung ensure that minimal effort is required during breathing and also that there is maximal compliance of lung, as well as easy clearance of alveolar fluid from the air/lung interface. • Over the last 3 months of gestation, alveolar surfactant is produced and stored and is secreted into the fluid-filled alveoli from specialized cells (Clara cells) that manufacture it. The amniotic fluid will necessarily therefore have significant levels of these complex proteins. • Endogenous corticosteroids, thyroid hormones and β-adrenergic agonists stimulate maturation and as these chemicals are a significant feature of the later developing fetus they prepare the lung for inflation. They also appear to cause a thinning of the alveolar cells thus tending to lead to an easier transfer of oxygen across the alveolar–capillary barrier from the point of birth. • The neonatal respiratory distress syndrome (see p. 275), which is commonly encountered in premature animals of all species, results from a failure of this complex mechanism to mature matched with delivery. Primary or secondary deficiencies in the supply or maturation of surfactant can arise. Primary deficiency leads to the characteristic fetal distress syndrome in which gasping and extreme respiratory efforts fail to alter the progressive anoxia and hypercapnea (see p. 275). The foal needs to rise quickly to its feet and to move with certainty (Fig. 1.3). This means that the muscles and skeleton must be well developed at birth and also adapted to rapid adjustment to the new forces and functions. Foals are able to stand well within 1–2 hours of birth and are usually capable of rapid movement within 2–4 hours. This adaptation also involves the nervous system, which has to perform a vast range of functions which have been only ‘tested’ in utero. It would be a major disadvantage if a full term foal were to practice and develop the full range of muscular activity in utero. There is some evidence that in utero movement of the foal becomes progressively more limited in the last months of pregnancy. Owners might therefore report that the foal’s movements have reduced or may even have apparently stopped altogether – suggesting that there may be a problem with the pregnancy. The limited movement in the later stages of pregnancy may predispose the relatively long-legged foal to abnormalities of growth and discrepancies between the bone growth (over which there is almost no control) and the tendon/ligament growth (which is probably coordinated by movement, posture and forces applied during their development). The lack of weight bearing within the uterine environment means that the skeleton and tendons/ligaments cannot adapt to forces and stresses and so it is perhaps surprising how efficient the system is. Nevertheless this may explain why a high proportion of foals are born with some form of flexural or angular deformity (see p. 289). The adaptations are, however, very rapid and even some severe ‘abnormalities’ correct spontaneously within days. Serious pathological abnormalities of the limbs and the axial skeleton will inevitably have a profound effect on the foal’s survival. Failure to rise will mean failure to feed and so death will be inevitable unless measures can be taken to provide support or treat the conditions, or both. The next obvious major adaptation is the change from placental nutrition to alimentation. In order for the foal to feed effectively (Fig. 1.4) it must first of all have a perception/instinct to rise and then to seek for the teat. Sight may be less important than is expected but it would obviously help! Having once located the teat it must already be in a position to suckle effectively and to swallow. Once swallowed the colostrums and milk must be delivered to the gastrointestinal tract and then digested efficiently. The timing of the first suck is critical for passive transfer of immunity (see p. 18) and because the foal has poor energy reserves (see p. 178). The composition of the mammary secretion changes considerably with time.8 In the first hours after birth the milk is rich in immunoglobulins (the secretion is even given a special name – colostrum). It is tempting to assume that milk provides all the nutritional requirements for the foal. However, in the longer term this is not necessarily so; foals need to supplement the milk feed with other ingesta within weeks of birth and will often be seen to take grass or hay within days of birth. Milk does, however, contain a delicately balanced variety of essential nutrients including vitamins, minerals and enzymes. Fats and lactose provide approximately equal proportions of the carbohydrate requirements for the foal and these must be digested by appropriate enzymatic/digestive processes. Therefore artificial milk replacers are unlikely ever to match the gold standard of normal milk for any particular species. Artificial milk replacers need to mimic the natural state as closely as possible (see p. 18) if digestive problems are to be avoided and so natural mare’s milk is used to provide the formula for the preparation of artificial milk supplements. Defecation is an important clinical feature. The waste material from the digestive processes which have also been going on during gestation and from ingestion of colostrum mean that the gut must be fully patent to the anus and that there should be no physical, neurological or other obstruction. Most foals will pass meconium (Fig. 1.5) within the first few hours and often within a few minutes of the first feed. Colostrum is thought to have a highly laxative effect and so is a significant benefit but it is unlikely that it will have any direct effect within minutes of ingestion. Feeding and perineal grooming by the mare stimulate rectal reflexes and encourage defecation. Meconium can easily be distinguished from the digestive products of milk. The former is usually pelleted, dark brown in color and has a very sticky consistency while the later usually is lighter yellow–orange in color and is a more fluid/pasty consistency. Figure 1.5 Meconium. This is significantly different from the milky/pasty feces of colostrum digestion. The clinical assessment of the alimentary tract of the foal is limited to the mouth and the anus and to the auscultation of the borborygmi that indicate progressive peristalsis. Probably the most significant initial clinical finding is the presence (or passage) of meconium (see p. 249). This indicates that the gut is patent and that neurological movement of the gut is normal. Atresia of a portion of the tract (see p. 104) or severe impairment of motility (see p. 103) will preclude any accumulation in the rectum and accumulation of ingesta proximally will result in painful distention and accumulation (see p. 249). While the normal foal has a defined demand for food materials the abnormal or sick foal will inevitably have an increased demand for all the components. The demand for energy is often at least 50% above normal and it can be much higher than this. The same applies to protein and fats as well as minerals and vitamins. Premature foals require extra food to complete organ maturation but infection; fever and cytokine release are extreme demands on the foal’s ability to ingest enough raw materials.9 In reality a sick foal often has a reduced appetite and so it can easily fall into a downward spiral. The specific requirements of the normal newborn foal are: The nervous system has an additional role in the adaptive period with the employment of the senses and mentation including maternal imprinting/recognition and behavior.10 The behavioral instincts in the first minutes are well described. Foals are usually non-responsive while they are within the birth canal but will respond to noxious stimuli such as gentle pressure over the eyelid or pinching of the hoof. The righting reflexes are activated before final expulsion and the normal foal usually adopts a sternal position within minutes of birth – this behavior improves breathing significantly (see p. 3). Significantly the menace responses are weak at birth and may remain so for some days postdelivery. The position of the eye also alters in the minutes after birth; the pupillary angle is ventromedial to the palpebral fissure and this becomes normal over the first week or so. There may be many reasons why a foal fails to behave normally, including blindness (see p. 135), central nervous system pathology such as the neonatal hypoxia–ischemia syndrome (see p. 166) and severe blood loss. Some foals may adapt more slowly than others and so rapid decisions should not be made where no pathology can be found. Foals may show apparent neurological difficulties as a result of pathology in other body systems. A foal may be born blind but normal vision may develop over 1–2 days after birth. It is remarkable that foals have poor eye reflexes at birth with poor menace responses (that may be mistaken for blindness) and low corneal sensitivity. It is important to remember that blindness may not be a result of central neurological problems – a bilateral dense cataract may cause obvious visual difficulties without any neurological implications. The latter may predispose the foal to corneal injury and even extensive corneal ulcers may not cause any overt pain or discomfort. The neonatal foal is born wet and even in the best of circumstances will have to withstand a thermal shock at the time of birth. The ambient temperature is rarely high enough to overcome heat lost by evaporation or by direct loss into the cold undersurface. The considerable muscular effort that foals exert at the time of birth will compensate for some of this but there is almost inevitably a fall in body temperature at birth.11 In spite of the necessity of maintaining a normal core temperature, foals can be born in very harsh conditions and suffer no ill effects at all; survival depends upon a rapid and effective adjustment to the environmental conditions and involves all the body systems adaptations. Healthy foals can usually cope with ambient temperatures as low as 5°C without significant problems. Native pony and horse breeds are well adapted to cope with their prevailing conditions but may be less able to cope when they are in unnatural surroundings (e.g. Thoroughbred foals in very cold conditions). Rapid adaptation and early feeding appear to be the most significant factors in survival in inclement conditions. Maintenance of body core temperature requires considerable energy demand; the only way that the newborn foal can supply this is by rapid mobilization of stored energy and fat. Healthy foals can restore and maintain normal body temperature without supplemental feeding for up to 12–24 hours, but where the foal either has poor reserves of energy or has an increased demand (such as occurs in sick foals) body temperature will drop significantly. Urinary excretion begins during gestation with passage of urine into the bladder and then into the allantoic space. A smaller volume of urine will pass into the amniotic fluid via the urethra. The mean urine production in a neonatal foal is around 145–155 mL/kg body weight per day.12 This figure is far higher than in mature horses. These factors can be explained simply by the fact that the neonatal kidney is not functionally mature at birth and so renal concentration of urine is much less efficient than in adult horses. Foal urine is frequently more dilute than that of adult horses. The naturally high fluid intake and the lack of concentration ability mean that foal’s urine has a naturally low specific gravity. The inability to concentrate urine means that it may remain relatively dilute in the face of dehydrating conditions that might otherwise be expected to cause urinary concentration. For the first 72 hours after birth, foals also often have a relatively high urinary protein concentration13 but this can be significant even in the normal foal. Although there is widespread fear of using renally excreted drugs in neonatal foals, most studies suggest that, at least with aminoglycoside antibiotics, the normal neonatal foal is probably mature enough to handle most of these. On a per kilogram body weight basis, the full term neonatal foal’s glomerular filtration rate (GFR) and effective renal plasma flow (ERPF) were determined to be comparable to adult values.11–14 However, use of these drugs is still questionable and dangerous in dehydrated and premature foals. In addition, other nephrotoxic drugs such as phenylbutazone may also damage the renal tissue of the immature kidney more than it would in an older horse. The first passage of urine is an important event with respect to neonatal assessment (see p. 88). Colt foals usually pass their first urine around 5–6 hours of age. In contrast, filly foals may delay their first micturition up to 10–11 hours. This has implications for those animals that have urinary tract defects. Ruptured or patent bladder syndromes are a relatively common event in foals and a few cases of uroperitoneum are also due to rupture of one or both ureters (see p. 255) (Fig. 1.6). Critical assessment of micturition and estimation of urine volume are therefore important aspects of neonatal management. Accumulation of urine within the abdominal cavity is not rapidly fatal and most cases are presented at between 36 and 72 hours of age when lethargy and abdominal distention are detected. Characteristic electrolyte and metabolite changes are presented (see p. 257). The color and content of the urine can be significant in many pathological conditions. For example, pigmenturia can be a result of myopathy (myoglobinuria) and can arise in foals with neonatal hypoxia syndrome foals with or without selenium or vitamin E deficiency (see p. 22), or both. Intravascular hemolysis results in varying degrees of hemoglobinuria and this is a possible sign of the neonatal isoerythrolysis and piroplasmosis syndromes. Frank blood in urine reflects hemorrhage into the urinary tract at some point from the kidney distally – this may arise from trauma or from clotting abnormalities such as hemophilia. The urachus is an important structure in the newborn foal. At birth the urachus is ruptured with the umbilical cord and some dribbling of urine is possibly normal in some foals. Persistent dribbling is probably abnormal (see p. 325) and many such cases have septicaemia (see p. 197). Infection of the urachus is always a significant disorder (see p. 330) and this can usually be identified clinically or by ultrasonographic examination of the region. Rupture of the urachus and seepage of urine into the periumbilical tissues cause severe damage locally (see p. 328). Management of the umbilicus is an important aspect of normal stud supervision (see p. 75). The adrenal cortex of the fetal foal is relatively quiescent for most of the latter part of gestation, but starts to rise during the last 4 days prepartum with a short rapid escalation in circulating cortisol preceding delivery (Fig. 1.7).15 Normal plasma cortisol in full term foals at birth is approximately 70–80 ng/mL.16 This rises dramatically in the first few hours of life to 120–140 ng/ml and then falls to around 60 ng/mL by 6 hours and reaches a baseline of around 30 ng/mL by 3 days (Fig. 1.7). Cortisol concentrations in premature foals are invariably much lower and this is not surprising, as the maturation of the adrenal cortex appears to be pivotal in the maturation of the fetus and its readiness for birth.17 Cortisol is important for many reasons including the final maturation of the surfactant–lung expansion mechanisms. In premature foals the plasma cortisol concentration may be as low as 20 ng/mL and this rises only slowly and only up to about 30 ng/mL in the next 2 days.18 In normal foals there is a rapid rise following administration of ACTH but in the premature foal this response is poor. The newborn foal has one of the highest concentrations of circulating thyroid hormones of the domestic animals.19 Thyroid hormones govern many metabolic and physiological functions. The metabolic rate and the normal development of individual body systems depend heavily on normal thyroid function. Most of the available T4 is converted to T3 and in late gestation the thyroid is stimulated strongly by a centrally driven mechanism (Table 1.1). At birth thyroid hormone concentrations are up to 10–20 times that of adult horses. T4 levels drop still further and T3 levels rise significantly over the first week of life and then fall back to normal levels by 4 weeks. High dietary iodine fed to the mare can result in an obvious goiter in a newborn foal. High iodine concentrations inhibit thyroid function, and foals with goiter (see p. 145) may be hypothyroid or may have normal levels of thyroid hormones. Fetal hypothyroidism occurs in neonatal foals and is characterized by weakness, tendon contracture, rupture of the common digital extensor tendons, tarsal and carpal bone softening/collapse syndromes, arthrogryposis and abnormalities of the face (‘squiffy face’, parrot mouth, etc.) (see p. 145).20,21 It is important to remember that these disorders may also have other causes. • In normal foals the blood glucose concentration at birth is about 3–3.5 mmol/L. This rises in the first 24 hours to over 4.5–6 mmol/L and should then be maintained through normal glucose homeostatic mechanisms by insulin and glucagons primarily. Endogenous catecholamines and glucocorticoids also have a significant effect on blood glucose concentrations in normal and abnormal foals. • Foals have relatively low stores of glycogen in myocardium and brain and mobilization of glucose is compromised in the newborn. The development of gluconeogenic enzymes in the liver and kidney of the newborn foal is poor at birth and function may only reach adult levels by approximately 1 month postpartum.23 Foals have glycogen stores to give them sufficient energy for only approximately 2 hours postpartum. Therefore this is another important reason, alongside passive transfer of immunity, why foals must suckle and drink colostrum within this time. • In premature foals the blood glucose concentrations are notably lower (2.3–2.7 mmol/L) and they consistently fail to maintain these levels adequately, with a steady drop in the first 2–4 hours of life. Failure to address this is a significant factor in the high mortality of premature foals. • Blood glucose concentrations form an important diagnostic and management tool for all intensive care foals. Failure to maintain adequate/normal concentrations results in depression and lethargy. Many intensive care procedures are less than effective if the blood glucose is not maintained. • Blood glucose can easily be measured using standard dry chemistry (stick) analyzers; although these are specifically designed for humans they do provide good accuracy in the foal. A comparison of gestation length for the pony, Thoroughbred and donkey is shown in Table 1.2. In Thoroughbreds normal gestation can be well in excess of 350 days and there are many reports of pregnancies of over 365 days resulting in a normal foal! A comparison of the mean and range of birth weights for colt and filly Thoroughbred foals is shown in Table 1.3. The adaptive period is the time during which the foal must adjust from the uterine environment to the ‘independent dependence’ of extrauterine life. The events occurring in foals over the first 72 hours of life are summarized in Table 1.4. The normal reference values for hematology and biochemistry in the foal up to 7 days of age are listed in Table 1.5. Table 1.5 Reference values for haematology and biochemistry of foals1 1From Knottenbelt DC (Ed) (1997) Formulary of Equine Medicine, University of Liverpool 2Changes faster if early cord rupture occurs 3Some foals less than 24 hours old without renal disease have creatinine concentrations between 530-2033 mm/L. It is wise to continue monitoring for the trend. 4Samples taken in lateral recumbency may be significantly higher (around 50 mmol/L is possible). Repeat check after sternal recumbency or standing is helpful. 5Samples taken in lateral recumbency may be significantly lower (around 75 mmol/L is possible). Repeat check after sternal recumbency or standing is helpful. The immune system has evolved to recognize and eliminate foreign molecules by use of exquisitely controlled intercellular responses to provide defense against pathogens. Survival against infectious disease depends upon adequate host defense mechanisms that include the complex of immune process and natural barriers to the invasion of pathogenic organisms. Under conditions of challenge the immune system must respond rapidly so that the pathogen can be eliminated before the host succumbs.
PERINATAL REVIEW
PERIPARTUM ADAPTATION OF THE FOAL
CARDIORESPIRATORY ADAPTATION
Lung maturity and surfactant development
LOCOMOTION
ALIMENTATION

NEUROLOGICAL FUNCTION
THERMAL REGULATION
RENAL FUNCTION
ENDOCRINE FUNCTION
Adrenal function
Thyroid function
Blood glucose concentration
REVIEW OF NEONATAL PHYSIOLOGY
NORMAL REFERENCE VALUES
Gestation Length
Thoroughbred birth weight
The adaptive period
Hematology and biochemistry
UNDERSTANDING IMMUNITY IN THE FOAL
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


PERINATAL REVIEW