CHAPTER 14 Parturition and Dystocia
The average gestation length in mares is approximately 340 days. There is considerable variation; gestation length may range from 315 to 400 days and is influenced by season, with pregnancies that terminate in winter longer than those that terminate in summer. When large variation occurs from the average there always should be some concern and the mare should be examined if indicated. The definition of eutocia is a “normal delivery” or as a safe easy delivery without significant injury to either the fetus or the mare.
MARE PREPARTUM CHANGES
Progesterone concentrations in the peripheral plasma are less than 1 ng/ml during the last half of gestation; thus, measurement of this hormone is useless for determining deficiencies or predicting the time of parturition.1 Other progestogens, 20α-hydroxy-5β-pregnan-3-one and 5β-pregnane-3α,20α-diol, decrease during the last 24 hours prior to parturition.2,3 Prepartum changes in the mare include enlargement of the udder 4 to 6 weeks prior to delivery. This time varies with the individual animal and is somewhat dependent on the number of previous pregnancies, if any. The udder becomes more rounded as it enlarges. Enlargement and edema of the udder and the abdominal wall immediately anterior to the udder are apparent 2 to 3 weeks prior to foaling. Waxing, or the appearance of a sebaceous-like secretion on the teat ends surrounding the sphincter, should occur as the mare approaches parturition. However, waxing has been observed to occur as early as 4 weeks prior to delivery and may not occur in some mares. Waxing generally occurs with regularity in the same animal at approximately the same time prior to parturition. The teats usually fill and distend 2 to 14 days prior to parturition, but this may not be observed. Some mares leak colostrum prior to parturition. This is undesirable because once the colostrum is lost from the udder it is not replaced. Colostrum should be collected and frozen or substitute colostrum should be made available for the foal following delivery.
Relaxation of the tailhead and pelvic ligaments occurs gradually over several weeks before delivery. During this same period the vulva relaxes and the opening elongates. At 1 to 3 weeks prior to foaling, relaxation becomes apparent in the flank area with the mare appearing somewhat “gaunt” in this area. Approximately 7 to 10 days later, the gluteal muscles and the muscles adjacent to the tailhead relax and appear less evident, with the bones in that area more pronounced. The ultrasonographic character of the fluids within the uterus also changes during the last 10 days of gestation, and echogenic particles appear. The vagina and vulva relax and there is an increase in mucus. The vaginal mucosa may appear reddened; this generally occurs within 24 hours of parturition. The cervix becomes completely relaxed and the uterine contractions increase in frequency and strength. Because some mares foal with only a few of these normal prepartum signs, prediction of the exact time of foaling is difficult without further diagnostic tests. Body temperature has been suggested as a possible method to determine the time of parturition before the onset of stage I of labor.4,5 Although it has been demonstrated that changes in body temperature measured at 6-hour intervals with an electronic rectal thermometer were not adequate to predict parturition, the use of telemetry with a computerized system to record core body temperatures at 15-minute intervals could be useful in parturition prediction.6,7
A number of methods commonly are used to monitor the actual parturition. The most frequently used and oldest method is to stay in the barn with the mare and personally observe. This method obviously has several disadvantages including inclement weather and loss of sleep. This system is not 100% effective, and many people have fallen asleep while supposedly observing the foaling or have gone to the house for a few minutes and have missed the birth. Others systems designed to improve the quality of life of the foaling attendant include video cameras, sound monitors, the Foal-alert system, the Birth Alert system, and other systems designed for the mare at parturition. Video cameras have progressed considerably from the days of the poor image quality requiring a great deal of light and hard wiring. The systems of today require minimal lighting and no wires. The cost of these systems also has been greatly reduced, making them affordable to most horse farms. They permit the person monitoring the mare to remain in a more comfortable environment than would otherwise be possible. The author has used several video monitoring systems over the past 22 years and has found them to be worth the cost. Sound monitors including baby monitors and intercoms are of limited value because many horse sounds may “wake” a horse owner and not be related to foaling. However, they do work in combination with other systems such as the monitors, which emit an audible signal at the time of parturition. The Foal-alert system is a monitoring device that includes the placement of a transmitter on the vulvar lips such that at the time of parturition the lips spread with passage of the fetus and the transmitter is activated. The receiver is activated and it produces an audible sound, which can be heard within the barn or transmitted by phone or pager to a distant point. An intercom system can also be used to transfer the alarm sound to a house or sleeping area of the foaling attendant. The Foal-alert system works excellently if any portion of the fetus or fetal membranes filled with fluids reaches the vulvar lips and causes activation of the transmitter. The Birth Alert system is another foaling monitoring system that utilizes a transmitter in the anterior vagina and is activated when the transmitter is expelled from the vagina and the temperature sensor signals the decrease in temperature to the receiver. The receiver transmits an audible signal.
Restlessness increases as the mare approaches parturition. Prior to this increase, mares may demonstrate decreased activity that could last for several weeks. Personality changes are obvious as the time of parturition approaches. This is especially true during the 24 hours before birth. Distractions of any kind should be kept to a minimum during this period. Changes in prepartum myometrial activity have been reported.8,9 Internally, during this period, the mare’s uterus begins more active contractions beginning at the end of the uterus near the ovary and progressing posteriorly toward the cervix.
The fetus is in a variety of presentations until approximately the sixth month of gestation when it aligns itself in a cranial presentation (Fig. 14-1). Presentation may change after this stage, however, and therefore cannot beused reliably to determine the presentation of the fetus until parturition actually begins. The fetus assumes a variety of positions, including dorsosacral, for longer durations as term approaches. As parturition approaches, the head and forelimbs can be palpated in the pelvic canal of the mare and may at times be alongside the cervix with pressure on the vaginal wall.
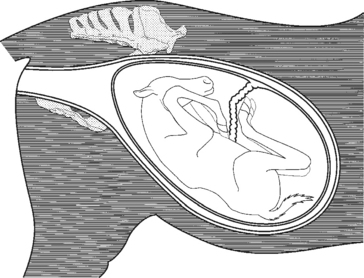
Fig. 14-1 Fetal presentation and posture 2 to 3 months before birth.
(From Threlfall WR: Threlfall’s equine obstetrics. Powell, OH: Global Reproductive Services, 1996.)
Stage I
Sweating initiated in the shoulder area combined with frequent observations of the flank area by the mare are indicators that stage I of labor is occurring. Kicking, biting of the flank, or other signs of mild colic frequently occur during this period. During this stage, final positioning and posturing of the fetus occur. The front feet and the nose make an excellent wedge to aid in cervical dilatation. This is also assisted by pressure of the fetal fluid on the cervical opening. The increase in pressure is first due to increased uterine activity. As the pressure increases and the cervix starts to dilate, oxytocin is released. Oxytocin increases the uterine contractions and indirectly stimulates the abdominal muscles to contract and further increase the uterine pressure. The beginning of stage I of parturition is difficult to determine because its onset is not marked by any single event or change in the mare and is rather vague and variable. As the normal mare approaches foaling, she may have a decrease in activity the day before the night of foaling. It has been reported that approximately 85% of mares foal between 7:00 PM and 9:00 AM, with most mares foaling between 11:00 PM and 4:00 AM.4 Within 2 hours prior to foaling, the mare may become restless and show signs of colic. She may paw the ground and stop eating for short periods of time as an indication of pain. Increased switching or movement of the tail is also usually observed as the mare approaches parturition. Milk may be seen squirting from the teats. This activity is associated with oxytocin release and apparent uterine pain. Signs of pain are not constant but intermittent and correspond with uterine contractions. These periods may last from 1 or 2 minutes to 20 minutes in length. These events may not be observed in older mares, even though the entire process may take several hours. This explains how mares are able to foal during the 30 minutes an observer may be absent. The mare should be observed but left undisturbed unless problems arise. The average range for this period is 1 to 4 hours. Any disturbances may delay the foaling and result in complications. The chorioallantoic membrane ruptures and the allantoic fluid escapes, marking the end of stage I.
Stage II
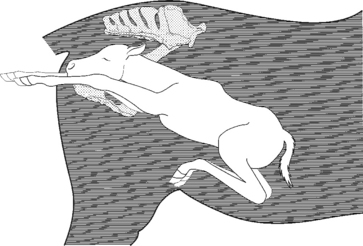
Signs of the second stage of labor are more apparent. The mare lies down during most of this period; although she may sit up and lie down several times and is generally sweating. When in the recumbent position, all legs may be extended and the head stretched outward away from the body (Fig. 14-2). She may bite her flank area or chew on hay or straw. During stage II of labor, the mare frequently urinates and defecates because of the pressure applied by the contracting uterus and the abdominal wall and the presence of the fetus and fetal fluids. Some mares may roll in an apparent attempt to lessen the pain or position the fetus. The average time for stage II is 20 minutes, calculated from the time of chorioallantoic membrane rupture until delivery of the fetus. It is abnormal for mares to continue this stage of labor longer than 70 minutes, and prolonged second stage indicates problems are present and fetal death is likely. It is generally recommended that mares be given 20 minutes to complete the second stage before the foaling attendant becomes alarmed. Normal progression in the delivery process should occur during this period.

Fig. 14-2 Mare in stage II of parturition with severe abdominal contraction resulting in all limbs extended.
(From Threlfall WR: Threlfall’s equine obstetrics. Powell, OH: Global Reproductive Services, 1996.)
During stage II, the amniotic membrane protrudes from the vulva (Fig. 14-3). The amniotic membrane should be visible at the vulvar lips within 5 to 10 minutes following rupture of the chorioallantoic membrane if the mare has not been disturbed during the delivery process. Once the amniotic membrane is visible, the fetus has entered the birth canal sufficiently to stimulate strong abdominal contractions. As the foal is pushed caudally by abdominal and uterine contractions, the feet are observed through the amniotic membrane. Rupture of the membrane does not usually occur until the fetus is at least midway or completely through the birth canal. Although most mares foal in lateral recumbency, it is possible for parturition to occur while the mare stands. The major concern in this situation is a ruptured umbilical cord close to the abdominal wall and blood loss. If the foal is delivered and the amniotic membrane remains intact as the foal struggles following delivery, the membrane should be incised and removed from the area of the fetal nose and mouth. The normal delivery posture of the fetus is one forelimb extending approximately 4 inches in front of the other and the soles of both feet directed ventrally (Fig. 14-4). This offsetting of the feet results in a slight angling of the shoulders and thereby reduces the width of this area as it passes through the mare’s pelvis. While the foal passes through the vulvar lips surrounded by the amnion, the observer can determine the offset position of the hooves and note that the soles are ventral. If the soles are not directed ventrally, immediate attention is indicated. The head should rest on the forelimbs in the area of the carpal joints. The head and neck are extended. If the nose of the fetus has not appeared by the time the carpal joints are observable immediate intervention is indicated. The vertebrae of the fetus are located near to the vertebrae of the mare; the position is close to a dorsosacral but slightly off toward the ileum. This position permits the fetus to take advantage of the greater pelvic diameter. As the fetus is expelled further, the rear limbs are extended so that the hooves are the last part of the fetus delivered. Any variation from this normal position, such as failure to observe one of the feet or the head and neck, indicates a postural abnormality and a difficult delivery. Because the mare’s delivery is so forceful, she may severely injure herself by pushing the fetus out and tearing her tissue as the fetus is expelled. Also, anything that slows the delivery process is detrimental because the placenta separates rapidly and eliminates the fetal supply of oxygen. This probably accounts for the poor survival rate of foals when the mare was in need of assistance and none was immediately available.

Fig. 14-3 Mare in stage II of parturition with the forefeet protruding covered by amniotic membrane.
(From Threlfall WR: Threlfall’s equine obstetrics. Powell, OH: Global Reproductive Services, 1996.)
Stage III
The mare should be permitted to lie quietly in the stall for up to an hour following parturition; however, if she jumps up rapidly following delivery, it is not necessarily a reason to panic. Although it has been suspected, it has not been demonstrated that abdominal wall damage occurs to the fetus when this occurs. The determination of hemorrhage from the umbilicus, although not common, should be made. It was once believed that large volumes of fetal blood could be lost from the placenta and that care should be taken to assure the cord remained attached to the placenta. A more recent scientific study revealed that blood flow through the umbilical vessels ceases by the time the umbilical cord is visible at the vulvar area of the mare.10 Following delivery of the fetus and after the mare has accepted the foal and is resting, cleaning of the stall and observation of the mare and foal are the two most important managerial tasks. Stage III of parturition begins following expulsion of the foal and ends when expulsion of the placenta is complete. The fetal membranes should be expelled within 3 hours following delivery.
INDUCED PARTURITION
The second reason for the induction of parturition is for convenience. Induction of parturition is becoming an acceptable method of permitting the owner, manager, or veterinarian to be present at the time of delivery in normal mares. The value of induced parturition in labor savings is brought about by the elimination of “foal watchers,” people hired to observe mares near term, or by the elimination of frequent observations throughout the night with the possibility of missing the foaling onset. The labor savings plus the guarantee that capable assistants will be present at the time of parturition easily offset the expenses incurred in parturition induction. The convenience factor also applies to certain research projects involving parturition and neonatal physiology and for the educational value of being able to provide a parturition demonstration. Induction has also been utilized to induce mares to deliver where the primary intention was to provide a nurse mare for a valuable foal. There is no association between induction and impaired future reproductive efficiency. Owners must be aware of the problems with dysmature or premature foals if delivery occurs prior to the time the foal is mature.
The most common agent used to induce parturition is oxytocin by intravenous or intramuscular administration.11 If the cervix is closed, administration of estradiol cypionate (4 to 6 mg) or diethylstilbestrol may be considered 12 to 24 hours in advance of oxytocin administration to aid in relaxation. Oxytocin also has the capability of inducing cervical relaxation in a mare with a closed or nearly closed cervix. The best results are obtained when it is administered as a 10-unit dose intravenously every 15 to 30 minutes by slow intravenous drip. Four to six repetitions of bolus administration may be required. If dilatation occurs without delivery, the dosage of oxytocin can be increased to 20 units. While determining the degree of cervical dilation, one can also determine the position and posture of the fetus by transrectal palpation because disruption of the mare has already occurred.
The dosage of oxytocin administered varies with the degree of cervical relaxation. If the internal diameter of the cervix is relaxed to at least 2 cm, it has been recommended by several authors to administer 40 to 60 units oxytocin as an intravenous bolus. Delivery of the fetus should occur within 90 minutes. In a pluriparous mare, the sequence may be more rapid, with stage II completed within 30 minutes after oxytocin administration. Many veterinarians have traditionally administered oxytocin intramuscularly.12 Much of the recent literature has reiterated the observation that the mare’s response (both in speed and violence) is proportional to the dose of oxytocin given. The higher the dose of oxytocin the faster the delivery of the fetus. Oxytocin has been reportedly used to induce parturition in six mares with all foals normal and healthy within approximately 34 minutes. None of the mares had a retained placenta and all lactated normally. The dose of oxytocin ranged from 40 to 60 units. The author prefers to administer 20 units of oxytocin intramuscularly to mares with a minimum of 2 cm cervical dilation and has not had any of the reported problems described later in this chapter.
Reportedly, oxytocin is dangerous when used to induce parturition because it has the capability to induce delivery whether the fetus is mature or not. The response of the mare is to release larger quantities of prostaglandin than occurs during a natural parturition and is therefore a pharmacologic not a physiologic induction. Fetal membrane retention occurred as an undesirable effect in two of three mares when oxytocin was given by slow intravenous drip for longer than 3 hours. Four of five mares induced with oxytocin produced foals that were weaker than normal, and one had to be “destroyed.” Cases of malposition have been reported following induction with oxytocin. It is recommended to examine the fetus 20 minutes following oxytocin administration to determine the fetal position and to correct any malposture or malposition. The author believes that all these side effects could and do occur in natural deliveries and that some of the effects may be related to dose or route of administration.
Prostaglandin F2 alpha (PGF2α) reportedly failed to induce parturition in the mare.13 PGF2α can also cause very strong myometrial contractions and may decrease foal survival and increase fetal weakness and risk of death due to early placental separation.13,14
Combinations of fenprostalene followed by oxytocin in 5-unit doses at 20-minute intervals has been recommended as a means to reduce the approximate 4-hour time interval following the prostaglandin analogue administration until delivery. Oxytocin was administered 1 hour following the initial injection and the delivery time was more predictable.12
Glucocorticoids have reportedly failed to induce parturition in the mare. Dexamethasone, 100 mg at 24-hour intervals until parturition occurs, has been utilized but with less reliability than oxytocin. The average induction time of 4 ± 1.6 days was considered to be undesirable because qualified assistance probably would not be present when required. Because suppression of the immune response is a disadvantage of corticosteroid therapy, it is thought that the use of this substance to induce parturition may be undesirable.13 Combinations of PGF2α and flumethasone, a synthetic glucocorticoid, have been reported to successfully induce parturition.
Dystocia
Next, the reproductive tract and fetus should be examined. The author prefers to perform this procedure initially via transrectal palpation. This approach permits evaluation of the uterine body more anteriorly than may be possible via the vaginal canal, thus allowing assessment of the existence of uterine torsion, rupture of uterine arteries, or uterine rupture on the dorsal surface. Fetal viability can also be assessed using the transrectal approach. The perineal area is then washed and, with the use of a sleeve and sterile lubricant, the vaginal, cervical, and uterine walls are examined for possible lacerations. This procedure should always be performed before examination of the fetus to eliminate the possibility of missing a significant lesion.
Intravenous general anesthesia can be safely performed in the field setting. The practitioner should review a contemporary veterinary anesthesia text for a more thorough understanding of the procedures involved and the potential risks of equine field anesthesia. Sedation with xylazine (1.1 mg/kg IV) is followed by induction with a combination of diazepam (0.06–0.1 mg/kg IV) and ketamine (2.2 mg/kg IV). This combination should provide approximately 10 to 15 minutes of anesthesia when used alone. The duration of anesthesia can be extended with administration of “triple drip” (also called GKX), which is made by adding 1 mg/ml of ketamine and 0.5 mg/ml of xylazine to 5% guaifenesin solution. Triple drip is administered at a rate of 0.08 to 1.6 ml/kg/hour IV (or 1–2 drops/sec/450 kg). The 1 drop/sec rate will generally extend recumbency, but will often not cover significant surgical stimulation later in the procedure. The 2 drops/sec rate will generally extend complete surgical anesthesia for the duration of the procedure. An infusion rate of 3 drops/sec has been reportedly used without adverse effects. A more stable plane of anesthesia will result if triple drip administration is started immediately following anesthetic induction. If field anesthesia must be extended beyond 1 hour, the second bag of triple drip should be made using half the concentration of xylazine to minimize the accumulation of this drug. Recovery from triple drip is generally very smooth and usually takes 15 to 30 minutes following short anesthetic periods. Expect recovery time to increase as anesthetic duration is extended. α2-Adrenergic antagonists (yohimbine, tolazoline) may be used to reverse some of the xylazine sedation to shorten these longer recovery times. They should be administered in small increments (0.005 mg/kg for yohimbine and 0.5 mg/kg for tolazoline) and not until the horse has been in sternal recumbency for some time to minimize the risk of a rough recovery. It is very important to be patient when using smaller doses of reversal agents to produce a titrated response. For best results doses should be given at 3- to 5-minute intervals.
Repeated bolus administration of xylazine-ketamine can be used as an alternative to triple drip for extending the duration of equine field anesthesia. One third to one half of the initial dose of each drug is administered intravenously as a bolus when signs of a lightened plane of anesthesia are observed. Xylazine dose should be systemically reduced when numerous boluses are required. The anesthetic plane achieved using this approach is not an even plane and requires more attention than when using triple drip.15
Obstetric equipment recommended by the author includes three obstetric chains (60 inch), three obstetric chain handles, fetatome (Utrecht or flat tube model), a Krey-Schottler hook, a wire introducer, two wire handles, a detorsion rod, a fetotomy finger knife, a rope snare, obstetric wire, a Kühn crutch, rubber sleeves, buckets, a stomach pump, a nasogastric tube, and lubricant. The lubricant of choice is polyethylene polymer (J-Lube*), ispolyethylene polymera which comes in powder form and is water soluble. It can be mixed at the site and delivered into the uterus with a stomach pump and tube. Although not all of this equipment is essential for every dystocia, its availability will improve the quality of the obstetric manipulation and reduce the work required to obtain desirable results.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


