Chapter 117 Miscellaneous Diseases of Bone
Some of the diseases affecting bone are discussed in this chapter. See respective chapters for other bone and cartilage diseases, such as hip dysplasia, avascular necrosis of the femoral head, and osteochondrosis.
PANOSTEITIS
Etiology
• Contributing causes include stress, transient vascular abnormalities, metabolic disorders, allergies, hyperestrogenism, and autoimmune reaction following viral infection.
Clinical Signs
Signalment
• Panosteitis usually is seen in large and giant-breed dogs, most often 5 to 12 months of age; however, it has been reported in dogs up to 5 years of age, and I have seen it in a 7-year-old dog.
• Male dogs are affected more frequently than females (4:1 ratio). In females, the first episode of the disease often occurs in association with the first estrus.
Lameness
• Pain due to the disease is of intermittent duration and severity, but the dog rarely, if ever, is completely non–weight bearing on the affected limb or limbs.
• Lameness or radiographic lesions may occur simultaneously in multiple limbs or bones, or lameness may resolve for a period of time, only to recur in another limb. After a bone passes through the lesion cycle, it is unlikely that it will be affected again, but lameness may occur in that limb if the disease affects another bone in the limb.
Diagnosis
Radiography
Confirm suspected cases by survey radiography of the affected bone(s).
• Early radiographic lesions are characterized by areas of increased density and accentuated trabecular pattern within the medullary cavity (Table 117-1).
• Bone cortices may be thickened, and progressive mottling and opacification of the medullary cavity occur.
• During resolution, sclerotic areas gradually decrease in size and density. Radiographic signs may persist for several months after lameness resolves.
Table 117-1 CHARACTERISTIC RADIOGRAPHIC LESIONS SEEN IN DISEASES AFFECTING BONE
| Disease | Lesion |
|---|---|
| Panosteitis | Increased opacity in medullary cavity of diaphysis |
| Hypertrophic osteodystrophy | Radiolucent metaphyseal line adjacent to physis |
| Hypertrophic osteopathy | Periosteal reaction beginning on metacarpals or metatarsals, bilaterally symmetric |
| Craniomandibular osteopathy | Bony proliferation on ventral mandible and skull |
| Cartilaginous exostosis | Large, smooth bony protuberance in metaphyseal area |
| Bone cyst | Well-circumscribed, radiolucent metaphyseal defect |
| Retained enchondral | Longitudinal, linear radiolucent cartilaginous core defect in distal ulna |
Differential Diagnoses
• Differentiate panosteitis as a cause of lameness from other diseases that are characterized by onset during or shortly after the rapid-growth phase in large-breed dogs.
• In particular, eliminate hypertrophic osteodystrophy, osteochondritis dissecans of the shoulder or elbow (see Chapter 118), ununited anconeal process (see Chapter 118), and hip dysplasia (seeChapter 108) as a cause of lameness before ascribing clinical signs to panosteitis.
HYPERTROPHIC OSTEODYSTROPHY
Etiology
• Historically, the disease has been attributed to vitamin C deficiency, but decreased levels of ascorbic acid in the serum or urine do not appear to be related to the disease.
• Skeletal lesions similar to those of HOD have been produced experimentally by feeding a free-choice diet abnormally high in protein, calories, and calcium.
Clinical Signs
Systemic Signs
• The severity of HOD varies, ranging from an absence of systemic signs to severe anorexia, weight loss, fever, and depression.
Diagnosis
Radiography
• Radiographic changes usually occur in the metaphyses of the long bones and are bilaterally symmetric. Other bones, including the mandible, ribs, and scapula, may be affected.
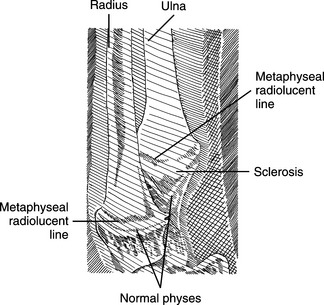
• The characteristic radiographic lesion is generalized sclerosis and enlargement of the metaphysis.
Radiolucent areas form in the metaphysis and coalesce to form an area of radiolucency parallel to the growth plate, called a double physeal line (Fig. 117-1).