Figure 56.2 Approximate location (dashed line) of the elliptical incision for mastectomy in an alpaca. Note that the lateral portions of the incision will preserve approximately 2 cm of dorsal mammary skin for closure after the gland in removed.
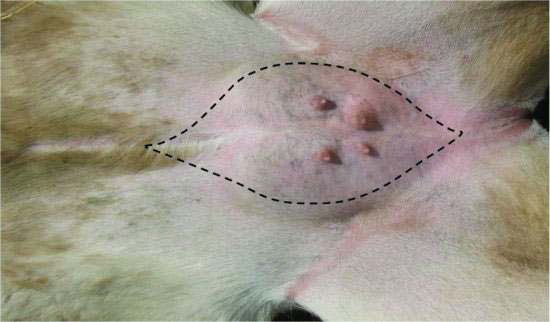
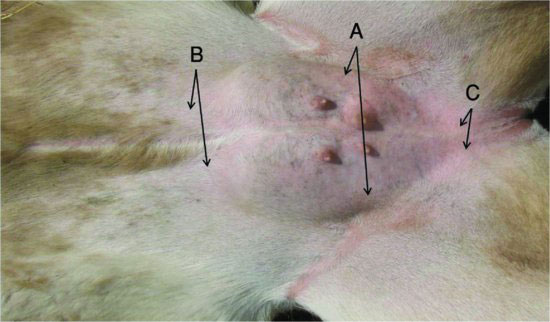
Figure 56.3 Approximate locations of the major blood vessels of the mammary gland. Paired pudendal arteries and veins (A) arise from the inguinal rings dorsal to the gland. Subcutaneous abdominal veins and branches (B) cranial to the udder and perineal arteries and veins (C) caudally.
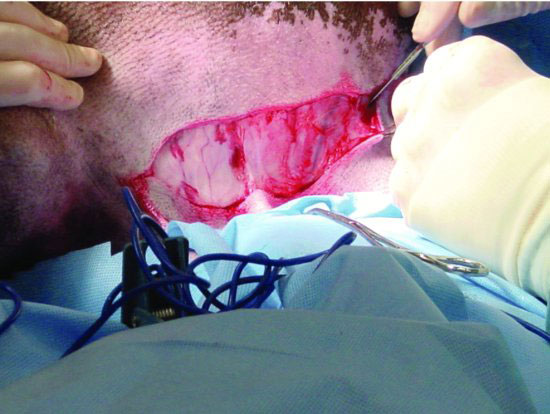
The external pudendal arteries and veins coursing along the lateral aspect of both sides of the udder should be isolated and ligated during the early phases of the procedure to limit blood flow into the udder and reduce intraoperative hemorrhage. A longitudinal skin incision is made on the lateral side of the udder and parallel to the abdominal wall, superficial to the inguinal ring, where it joins the abdominal skin. Preserve about 2 cm of the dorsal mammary skin to facilitate primary closure. The length of the incision is parallel to the skin attachment of the udder to the body wall. The incision will eventually be an ellipse surrounding the udder in later steps, and enough tissue must be retained for appositional closure (Figure 56.4). Continue the approach carefully through the subcutaneous fat and lateral suspensory ligament toward the inguinal ring. Frequently palpate for the pulse of the external pudendal artery to avoid inadvertent cutting trauma of the artery and vein, which lie just deep to the suspensory ligament and in close approximation with one another. (See Figure 56.5.) Isolate and ligate the external pudendal artery first, followed by the vein near the inguinal ring before these vessels bifurcate (Figure 56.6). By ligating the artery first, circulatory blood volume is preserved by allowing the udder to drain into circulation. Use of absorbable suture material is indicated. Braided suture are preferred to ensure holding power on tissues while tightening. Double ligation of the arteries using No. 2 chromic gut or No. 1 braided suture such as PGA-910 are desirable. Transect the vessels and check for bleeding. Repeat these first steps on the opposite side.
Figure 56.4 Initial incision is made on the lateral side of the udder preserving a portion of dorsal skin for closure. Continue approach through the lateral suspensory ligament to the inguinal ring.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


