Chapter 55 Management of the Traumatic Wound by Primary Closure
Following proper initial management of a traumatic wound by debridement and lavage, the wound may be closed. Sufficient viable tissue must be present to allow closure without excessive tension. Wounds may be closed by primary closure, delayed primary closure, or secondary closure. See Chapter 56 for a discussion of open wound management.
ANATOMY
• Dogs and cats have abundant skin on the trunk and neck but a sparsity of skin on the distal limbs, tail, ear, and rostral areas of the head.
• Direct cutaneous vessels run parallel to the skin’s surface and supply the subdermal plexus of the skin. See Chapter 57 for more details regarding blood supply to the skin.
• Some areas of the body have panniculus musculature underlying the skin. The skin’s blood supply runs both superficial and deep to this musculature.
PREOPERATIVE CONSIDERATIONS
• Perform a thorough physical examination and appropriate diagnostic tests on all traumatized animals to rule out associated injuries.
• Perform delayed primary closure when:
• Wounds show evidence of heavy contamination, purulent exudate, residual necrotic or questionable tissue, edema, erythema at the wound margins, lymphangitis, and skin tension.
SURGICAL PROCEDURES
Primary or Delayed Primary Closure without Tension
Equipment
• Undyed polyglactin 910, polyglecaprone, dyed or undyed polydioxanone, 2-0 to 4-0 (Vicryl, Monocryl, or PDS II; Ethicon, Somerville, NJ.) and polypropylene or nylon, 2-0 and 3-0 (Prolene or Ethilon, Ethicon, Somerville, NJ.)
Technique
1. Pack the wound with sterile surgical sponges moistened with physiologic saline, or with water-soluble sterile lubricant (K-Y Jelly, Johnson & Johnson, New Brunswick, NJ.) or water-soluble sterile lubricant that contains chlorhexidine gluconate (Surgilube, E. Fougera & Co., Mellville, NY.)
4. Lavage the wound frequently with sterile isotonic fluids (or a solution of 0.05% chlorhexidine diacetate or gluconate) during surgery along with removal of devitalized tissue and debris as indicated.
5. Use as few simple interrupted absorbable sutures as necessary to close dead space in deep layers of the wound.
7. Place a drain (Penrose drain, or a closed suction drain [Jackson-Pratt]) if there is any possibility of residual dead space and/or wound drainage.
8. Place a simple continuous suture in the subcutaneous tissue at the wound edge using absorbable suture material.
Postoperative Care and Complications
• Postoperative care
• Place absorbent surgical sponges over the suture line, with extra sponges over the end of a Penrose drain.
• Change the bandage every second or third day if there is no concern about possible complications. Change the bandage daily if there is concern about possible complications and/or a drain has been placed. The amount and nature of drainage should be assessed at each bandage change.
• Remove the drain and discontinue bandaging when the drainage becomes minimal and is the same in quantity at successive bandage changes.
Primary, Delayed Primary, or Secondary Closure with Tension
Technique
1. The general techniques for closure of wounds with tension are the same as those for primary or delayed primary closure without tension (see previous section), with the exception of suture pattern (see tension-relieving suture patterns discussed subsequently).
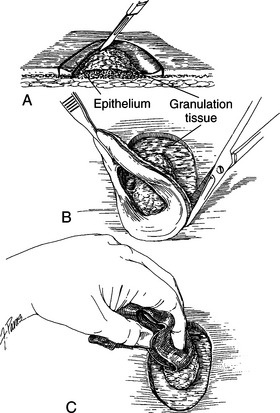
2. Wounds that are in the reparative stage of healing with healthy granulation tissue and epithelialization.
3. Gently undermine the skin surrounding the wound.
a. Undermine bluntly, using Metzenbaum scissors, leaving some loose areolar connective tissue on the dermis or undermine beneath panniculus musculature if present.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


