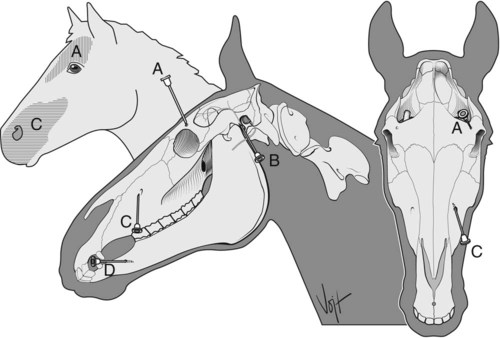
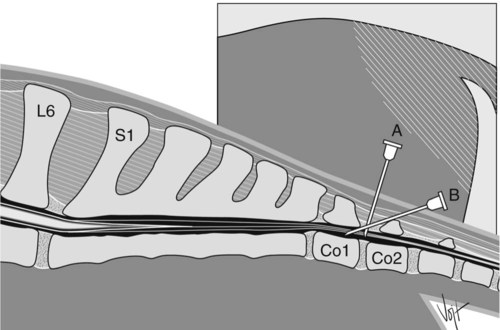
I Anesthesia of the upper eyelid and forehead A Area blocked: upper eyelid except medial and lateral canthi B Nerve blocked: supraorbital (or frontal) nerve C Site: supraorbital foramen (Fig. 6-1, A) D Needle: 22- to 25-gauge, 2.54-cm E Anesthetic: 5 mL of 2% lidocaine F Method: palpate the supraorbital foramen approximately 5 to 7 cm above the medial canthus where it perforates the supraorbital process of the frontal bone; insert the needle into the foramen to a depth of 1.5 to 2 cm; inject 2 mL of lidocaine into the foramen; 1 mL as the needle is withdrawn and 2 mL subcutaneously over the foramen A Area blocked: paralysis of orbicularis oculi muscles; no desensitization B Nerve blocked: auriculopalpebral nerve (Fig. 6-1, B) C Site: caudal to posterior ramus of the mandible D Needle: 22- to 25-gauge, 2.54-cm E Anesthetic: 5 mL of 2% lidocaine F Method: insert the needle into the depression caudal to the mandible at the ventral edge of the temporal part of the zygomatic arch; inject local anesthetic subfascially as the needle is withdrawn G Use: examining the eye; successful blockade of the motor nerve supply prevents the horse from closing the eyelids III Anesthesia of the upper lip and nose A Area blocked: upper lip and nostril, roof of nasal cavity, and related skin up to the infraorbital foramen B Nerve blocked: infraorbital nerve C Site: external opening of the infraorbital canal (Fig. 6-1, C) D Needle: 20- to 25-gauge, 2.54-cm E Anesthetic: 5 mL of 2% lidocaine F Method: insertion site is halfway along the bony lip of the infraorbital foramen, about 2.5 cm dorsal to a line connecting the nasomaxillary notch and the rostral end of the facial crest; push upward with the fingertips the flat levator labii superioris muscle, which runs over the foramen, and place the needle tip at the foramen opening G Use: treating simple lacerations in quiet or sedated horses IV Anesthesia of the lower lip and premolars A Area blocked: lower lip, all parts of mandible rostral up to and including the third premolar tooth (PM3) B Nerve blocked: mandibular alveolar nerve C Site: within mandibular canal (Fig. 6-1, D) E Anesthetic: 10 mL of 2% lidocaine F Method: palpate the lateral border of the mental foramen as a ridge along the lateral aspect of the ramus in the middle of the interdental space; insert the needle into the foramen as far as possible in a ventromedial direction; injection requires pressure, and fluid might partially drain back from the canal under the skin G Use: treating simple lacerations in quiet or sedated horses. The technique is difficult, so tooth extraction is better done with the animal under general anesthesia. A Area blocked: tail, perineum, anus, rectum, vulva, vagina, urethra, and bladder B Nerves blocked: coccygeal and last three pairs of sacral nerves C Site: epidural space in the first intercoccygeal space (Co1 to Co2) (Fig. 6-2) D Needles: spinal with stylet (spinal: 18-gauge, 5.1- to 7.6-cm) E Anesthetic: 6 to 10 mL of 2% lidocaine; other drugs can be considered (see Table 4-2) 1. Use proper restraint, depending on the horse’s temperament; clip, surgically scrub, and disinfect the injection site; make a skin wheal and infiltrate the tissues down to the interarcuate ligament with 1 to 3 mL of 2% lidocaine to minimize movement while inserting the spinal needle 2. Method A (see Fig. 6-2, A): insert the spinal needle into the epidural space in the center of the first intercoccygeal space (about 5 cm cranial to the origin of the first tail hairs and the caudal fold of the tail) at a right angle to the general contour of the croup and press the needle ventrally in a median plane until it strikes the floor of the vertebral canal; withdraw the needle about 0.5 cm 3. Method B (see Fig. 6-2, B): insert the spinal needle about 2.5 cm caudal to the first intercoccygeal space and slide its point ventrocranially at an angle of about 30 degrees to the horizontal plane and to its full length into the vertebral canal 4. Test with a syringe of air for resistance to the injection; alternatively, fill the needle hub with isotonic saline solution and manipulate slightly until the solution is aspirated from the needle by subatmospheric epidural pressure (hanging drop technique); inject local anesthetic; needle can be left in place with stylet reinserted; maximum blockade may require 10 to 30 minutes, and it is not advisable to redose during this time if surgery is to be done with the horse standing 1. Anesthesia of pelvic viscera without loss of hind leg motor control during obstetric manipulations 2. Anesthesia of genitalia without loss of hind leg motor control during obstetric manipulations 3. For standing surgical procedures of viscera and genitalia H Common causes for inadequate anesthesia or incomplete block 1. Improper injection technique 2. Inappropriate angulation of the spinal needle 3. Horses that have fibrous connective tissue from previous epidural injections, which limits diffusion of anesthetic agent
Local Anesthesia in Horses
Overview
Regional Anesthesia of the Head
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree