44 LMN paresis and paralysis
Acquired myasthenia gravis
INTRODUCTION
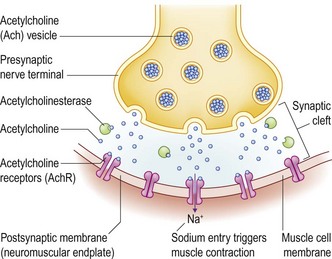
In the normal animal, the arrival of an action potential in a nerve terminus causes the voltage-gated calcium channels to open. The calcium influx induces a coordinated release of acetylcholine (Ach) into the synaptic cleft. The Ach binds to the Ach receptor on the skeletal muscle endplate, opening the membrane to sodium ions which depolarizes the post-synaptic membrane. Muscle contraction follows. The enzyme acetylcholinesterase rapidly removes the Ach from the synaptic cleft, allowing depolarization to recur (Fig. 44.1).
CLINICAL EXAMINATION
The dog was alert and could stand without assistance (Fig. 44.2). She quickly developed an arched back, all her limbs extended, and she quickly sat and then lay down. Proprioception was normal. Hopping was normal in those brief periods of standing. Spinal reflexes were normal to increased. Muscle tone was normal. No atrophy or muscle pain was noted. Pain perception appeared normal in all limbs. The blink reflex was weak bilaterally with the lids only partially closing. Facial sensation was normal.

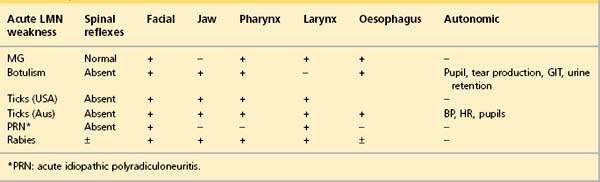
DIFFERENTIAL DIAGNOSIS OF ACUTE LMN SIGNS
Immune-mediated myasthenia gravis
Signs reflect skeletal muscle weakness and may be focal (facial, pharyngeal, laryngeal, oesophageal) or generalized (focal signs + appendicular/axial weakness). The most common initial signs in dogs are generalized weakness with megaoesophagus or megaoesophagus alone. In one study, 13% of seropositive dogs had generalized weakness without oesophageal or pharyngeal weakness. Cats chiefly present with generalized weakness and a decreased palpebral reflex. Extraocular muscle weakness is not reported in the small animal. Acquired myasthenia gravis is more common in the dog than the cat.
Signs may worsen with cold weather, oestrus cycles, pregnancy, concurrent infection and vaccination.
Tick paralysis
Diagnosis is aided by clinical improvement seen after tick removal. Engorged ticks may have fallen off by the time the animal is presented.
Acute idiopathic polyradiculoneuritis
Diagnosis is aided by finding an elevated level of total protein in the lumbar spinal fluid, reflecting the position of the nerve roots within the subarachnoid space (Table 44.1). Widespread denervation potentials are recorded on electromyography (EMG).
Polymyositis
Autoimmune polymyositis
is an autoimmune disease of unknown aetiology mostly affecting adult large breed dogs of either sex. Infectious myopathies caused by protozoa or tick-borne pathogens are rare but efforts must be made to rule them out with serology. Equally, drug-induced myopathies should be considered when taking a history. Paraneoplastic myopathies are rare. A generalized immune mediated disease may present as polymyositis.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


