Figure 39.2 Proper animal restraint and ultrasound placement for visualization of the liver and for subsequent biopsy.
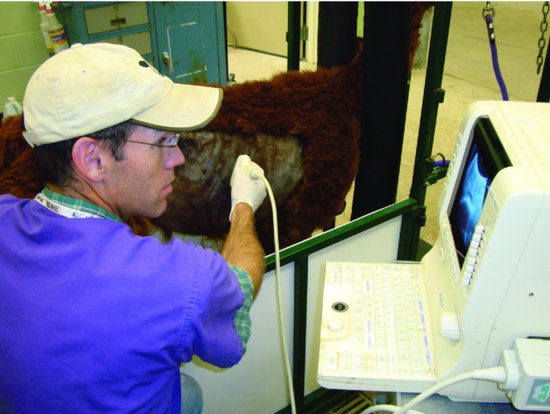
Figure 39.3 Ultrasound image of liver. Note the depth of the body to the liver surface and the depth to major blood vessels. The cm guides on the biopsy instrument can be used to ensure that the sample is taken within the hepatic parenchyma.

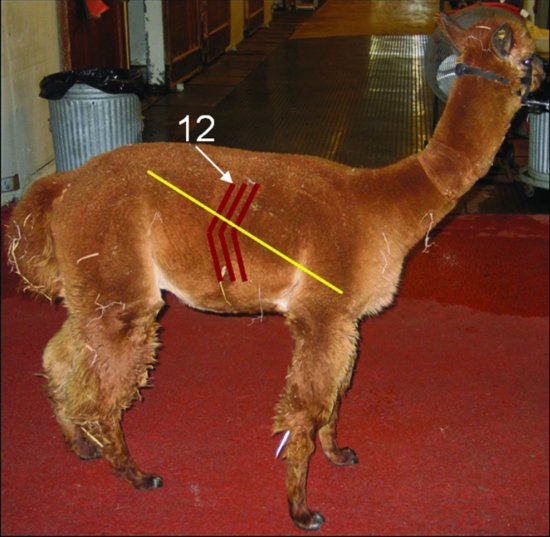
Figure 39.4 The site for blind liver biopsy is at the intersection of a line drawn from the ileal wing to the mid-humerus on the right side and the ninth or tenth intercostal space.
After preparation of the ultrasound guided or blind site, a small stab skin incision (0.5 cm) may be made and the closed biopsy instrument inserted in the intercostal space immediately cranial to the rib. This is selected because the vasculature and intercostal nerve courses along the caudal border of each rib. The needle is directed in a ventromedial direction until the liver is penetrated (Figure 39.5). At this location, the instrument penetrates the caudal thoracic cavity, the pleura, and the diaphragm prior to entering the liver. Caution should be used in tachypneic camelids because extreme caudal excursion of the lung may result in inadvertent penetration by the biopsy instrument.
Figure 39.5 Use of an automatic biopsy instrument in an alpaca. The instrument is placed off the cranial border of the rib and is directed ventromedially.

The operator will have a sense of the instrument entering a dense, spongy tissue. Some describe it as a gritty or coarse feel. Occasionally, the patient will involuntarily and suddenly move when the peritoneum and/or capsule of the liver is penetrated. Once into the liver parenchyma, automatic instruments may be triggered and withdrawn. For manual instruments, the obturator should be extended, the handle advanced to close the sheath over the obturator, and the instrument removed. The liver sample should be within the chamber. (See Figure 39.6.) If liver tissue is not present in the chamber, repeat the procedure by redirecting the instrument slightly until a sample is obtained. Samples may be placed in evacuated tubes for trace mineral analysis (and frozen if necessary), formalin for histopathology or sterile tubes for bacterial, viral, or fungal culture.
Figure 39.6 Typical appearance of liver tissue within the chamber of a biopsy instrument. This is best removed from the chamber using a needle.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


