TECHNICAL DESCRIPTION OF PROCEDURE/METHOD
Preparation
The hair should be clipped with #40 clipper blades and aseptically prepared for surgery. The clipped and prepared area should be four times the surface area of the operative site in order to provide wide margins for maintenance of a sterile field. In general, the preparation site should extend from the ventral midline to the dorsal midline.
Approach
A ventral midline approach to the abdomen is the standard method used in monogastric species for access to abdominal viscera. Anatomic differences require paralumbar fossae laparotomy for many problems in ruminant species. South American camelids have many clinical and anatomical similarities to ruminants. However, llamas and alpacas do not possess a distinct paralumbar fossa as is found in cattle, sheep, and goats. In camelids, the abdominal wall is tapered without a pronounced flank. Thus, laparotomy is described as being done from a lateral approach. The laparotomy incision may be made perpendicular to the spine (midlateral laparotomy), may follow the curvature of the last rib (paracostal laparotomy), or may be angled along the border of the internal abdominal oblique muscle at approximately a 30-degree angle caudal to the midlateral laparotomy site (caudal oblique laparotomy; Figure 42.2). The decision for left- versus right-sided lateral approach is based on the viscera to which access is needed (Table 42.1). The tissue layers involved in the approach to the abdomen through a lateral abdominal approach include the skin, minimal subcutaneous tissues, external abdominal oblique muscle (Figure 42.3), internal abdominal oblique muscle (Figure 42.4), transversus abdominus muscle, and peritoneum (Figure 42.5). From the right lateral abdominal approach, the pyloric antrum of C3 (Figure 42.6), jejunum and ileum (Figure 42.7), and cecum and spiral colon (Figure 42.8) can be readily exteriorized. As compared to the ventral midline approach, the most significant advantage of the right lateral abdominal approach is the ease of access to the duodenum (Figure 42.9), pancreas (Figure 42.10), and right kidney (Figure 42.11). The left lateral approach gives ready access to the spleen, C1, and left kidney.
Table 42.1 Differences in desired incision site for visceral access in llamas and alpacas.
| Right Side | Left Side | |
| Paracostal Laparotomy | Liver Right crus of diaphragm Pyloric antrum of third forestomach compartment (C3) Pylorus and duodenal ampulla Duodenmu Pancreas | First forestomach compartment Left crus of diaphragm |
| Midlateral Laparotomy | Pyloric antrum and fundus of third forestomach compartment Duodenum Jejunum Ileum Cecum Spiral Colon Right kidney Uterus Right ovary | First forestomach compartment Spleen Left kidney Uterus Left ovary |
| Caudal Oblique Laparotomy | Uterus | Uterus |
Figure 42.2 Laparotomy incisions through the lateral abdominal wall may be made via a perpendicular incision, paracostal incision, or a 30-degree oblique position.
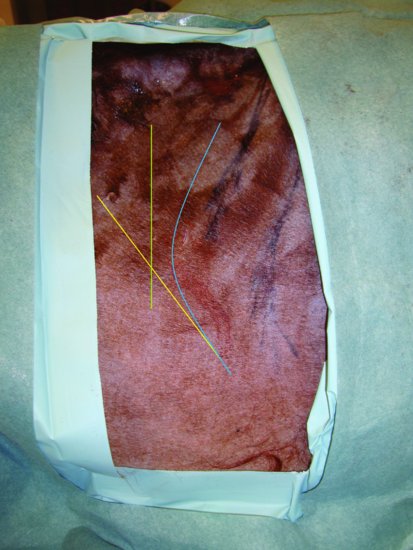
Figure 42.3 After the skin incision has been made, the external abdominal oblique muscle is visible.

Figure 42.4 The muscle layers in alpacas and llamas are thin with minimal fascial coverage compared with other livestock.

Figure 42.5 The abdomen is exposed after incising the external abdominal oblique, internal abdominal oblique, and transversus abdominus muscles.

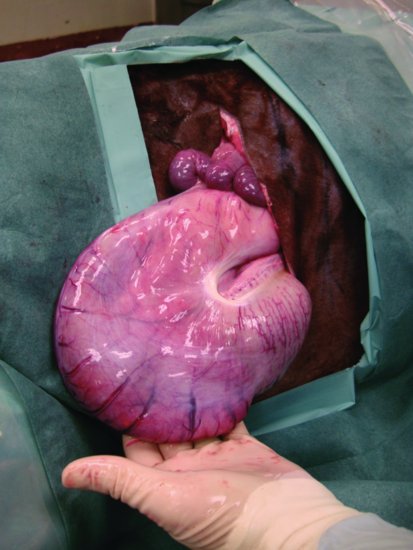
Figure 42.6 The distal portion (pyloric fundus) of C3 can be exteriorized from the abdomen and inspected for impaction, gastric ulcers, and other pathology.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


