Intramuscular (IM) injections may be made into the caudal cervical epaxial muscles or into the semimembranosus, semitendinosus, or triceps muscles. In the cervical region, the operator should palpate the region to locate the site of greatest muscle mass (Figure 6.2). The needle is inserted perpendicular to the skin and into the center of the muscle mass (approximately 3/4 inch to 1 inch [1.9 to 2.5 cm] in an adult), the plunger pulled back for aspiration, and, if no blood is seen in the hub of the needle, the injection given.
Figure 6.2 Placement of an intramuscular injection into the cervical epaxial musculature. Generally, no more than a 1-inch (2.5-cm) needle is used. The needle is directed perpendicularly to the skin into the muscle followed by aspiration and, if no blood is seen, the injection performed.

Intradermal (ID) injections are typically given in the fiberless area behind the elbow, on the lateral thoracic wall. A tuberculin needle is superficially inserted to remain within the dermis (Figure 6.3) and the small volume of biologic administered. The skin on the underside of the tail may be used, but camelids do not have a well-defined caudal tail fold, making ID injections in this area less desirable as compared to cattle.
Figure 6.3 Placement of an intradermal injection in the fiberless region behind the elbow. The tuberculin needle is directed at a shallow angle into the dermis and the injection performed.

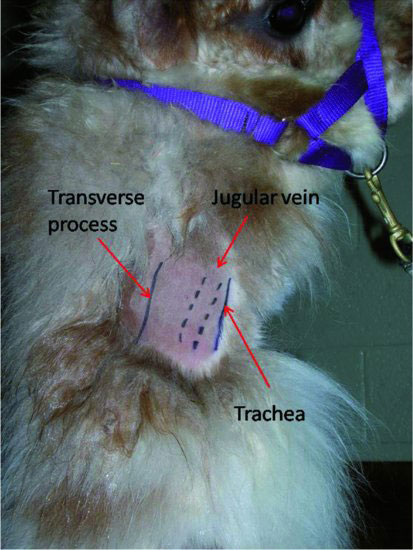
Intravenous (IV) injections are most commonly administered into the jugular vein, although the lateral saphenous and cephalic veins may also be used. The jugular vein is most easily injected in either the upper one-third (high venipuncture) or lower one-third (low venipuncture) of the neck. The mid-portion of the neck is easily accessed, but the carotid artery lies closer to the jugular vein in this region. Thus, caution should be exercised for mid-cervical injections. At the high (proximal) site, the skin is thinner than in the mid-cervical region, and the vein is superficial and somewhat separated from the carotid artery. At the low (distal) site, the carotid is close to the jugular, and there is increased risk of intra-arterial injection. However, the landmarks for puncture of the jugular vein can be easily palpated, and the vein is larger in this location. For both sites, the head and neck should be held upright and the animal well restrained. The operator should palpate the transverse processes of the cervical vertebrae and the trachea medially. The jugular groove lies between these two structures (Figure 6.4), and the vein is rarely visible, particularly when the animal is not clipped. The operator occludes the jugular groove using their thumb, bridging between the transverse process and the trachea, waiting to allow the vein to fill. The vein is then balloted with the opposite hand to confirm position and fill. The needle is inserted at a 45- to 60-degree angle into the skin. After the needle is into the soft tissues of the neck, the plunger is held with negative pressure as the needle is advanced and inserted into the vein (Figure 6.5). It is common to insert the needle through and deep to the vein. If this is suspected, negative pressure should be maintained as the needle is withdrawn and re-enters the vein. When blood is easily and consistently aspirated, the injection may be made. For larger volumes of infusion, an intravenous catheter should be used or an extension set attached to the needle to connect the needle to the syringe to prevent dislodging the needle and perivascular extravasation of the drug.
Figure 6.4 Location of the jugular vein within the jugular groove, lying between the transverse processes of the cervical vertebrae laterally and the trachea medially.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


