Table 28.1 Instrument requirements for inguinal herniorrhaphy in foals
| Surgical table capable of tilting to 20°–30° |
| Anesthetic machine with positive-pressure ventilator |
| Standard (general) surgery pack |
| Insufflator and CO2 source tubing |
| Light source, light cable, video camera, camera control unit, and monitor |
| 30° 10 mm telescope (33 or 57 cm—shorter telescope generally more convenient) |
| Cannulas (5 × 10 × 150 mm or 1 × 10 × 150 mm [telescope] and 4 × 5 × 150 mm [instrument]) |
| 1–2 aggressive laparoscopic grasping forceps (e.g., Semm) |
| 1–2 atraumatic laparoscopic grasping forceps (e.g., Babcock or Dorsey) |
| Laparoscopic scissors |
| Laparoscopic needle holders (2 × 33 cm or 45 cm) |
| Ligating loop knot pusher with insert sleeve and ligature loops of 1 USP absorbable suture |
| Optional: |
| Electrocautery unit with monopolar or bipolar handpieces |
| or |
| Advanced bipolar or electromechanical instrument (e.g., LigaSure™ or equivalent or ultrasonic shears) |
| Laparoscopic hernia stapler (requires a 10- to 12-mm cannula depending on the manufacturer) |
USP, United States Pharmacopeia.
Surgery
Portals
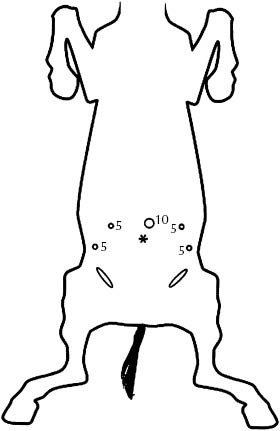
Abdominal access is achieved using an open approach 2–3 cm lateral to the umbilicus to avoid the urachal remnants. After a 10-mm telescope portal is made, and an exploratory examination is conducted to detect any other abnormalities, the foal is moved into the Trendelenburg position, and pneumoperitoneum is established with CO2. An intra-abdominal pressure of 8–10 mmHg is generally sufficient. When intracorporeal sutures are used for the herniorrhaphy, four instrument portals are made: one in the left abdominal wall approximately 5 cm lateral to the telescope portal and one 8–10 cm lateral and 4 cm caudal to the first instrument portal, an arrangement that is duplicated on the foal’s right side (Figure 28.2). These portals can be made to accommodate 5- or 10-mm cannulas; the author prefers the former. Importantly, the caudal-most portals should be made to allow a laparoscopic needle driver to approach the internal inguinal ring as closely as possible to parallel to its long axis.
Figure 28.2 Schematic representation of portal placement for the treatment of congenital inguinal/scrotal hernia in foals. A 10-mm periumbilical telescope portal is supplemented by four instrument portals, placed in a manner to optimize ergonomics of either endostapler or laparoscopic needle drivers. Four 5-mm portals suffice for intracorporeal suture closure of the inguinal rings; however, one or more of these portals must be equipped with a 12-mm cannula to accommodate a laparoscopic stapler. The asterisk represents the umbilicus.
If it is elected to conduct the herniorrhaphy using a laparoscopic stapling device, a 10- to 12-mm instrument portal on one or both sides of the abdomen has to be created to accommodate the stapler (the manufacturer’s directions provide the specific cannula size required). The location of this portal(s) should be such that the stapler can be oriented as closely as possible to perpendicular to the long axis of the inguinal rings, taking into account that most staplers can deliver staples with articulating angles from 20° to 60°.
Anatomy
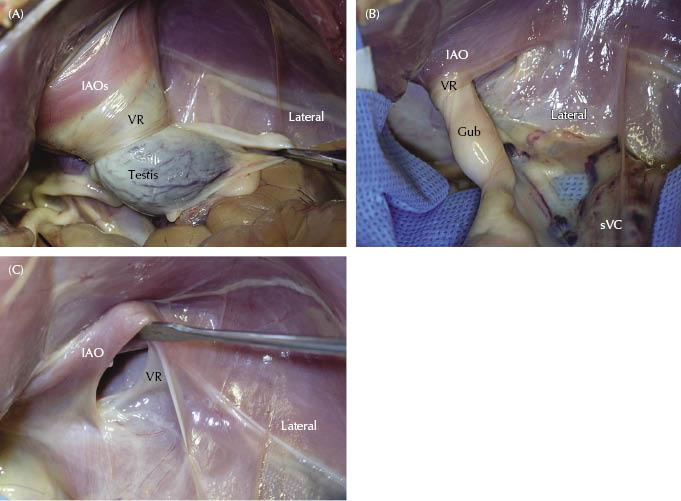
The regional anatomy will be familiar to most who have conducted laparoscopic cryptorchidectomy in anesthetized recumbent horses. The pertinent anatomical structures are shown in Figure 28.3.
Figure 28.3 Cadaveric dissection of a neonatal colt foal depicting the anatomy in the area of the right internal inguinal ring. (A) Traction on testicle (testis) causes it to protrude into the abdominal cavity through the elastic vaginal ring (VR). (B) Fully retracted testicle reveals the gubernaculum traversing the vaginal ring. (C) Vaginal and internal inguinal rings with gubernaculum and the nearby mesorchium and mesoductus removed. (The opening to the inguinal canal is being held open with a handheld retractor.) IAO, internal abdominal oblique muscle; Gub, gubernaculum; sVC, vascular cord.
Herniorrhaphy
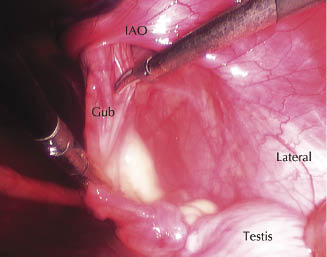
In most foals with intact vaginal tunics, bowel within the inguinal canal reduces spontaneously during Trendelenburg positioning. In foals with a ruptured scrotal hernia, the herniated small intestine is reduced by grasping and applying traction with atraumatic endoscopic forceps (Figure 28.4). In some affected foals, the testicle is located intra-abdominally, while in others, it can be withdrawn from a scrotal or inguinal location with gentle traction on the spermatic cord. Laparoscopic scissors or ultrasonic shears/advanced bipolar cautery forceps are used to transect the gubernaculum at the level of the internal inguinal ring bilaterally (Figure 28.5). The ductus deferens, mesoductus, and mesorchium are dissected free in the area of the inguinal rings leaving the vascular cord as the sole remaining testicular attachment. The testicle is relocated cranially to fully expose the internal inguinal and vaginal rings.
Figure 28.4 Reduction of an herniated intestine through the left inguinal ring of a foal with a ruptured scrotal hernia using atraumatic laparoscopic (Dorsey) forceps. IAO, internal abdominal oblique.
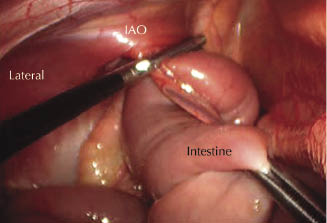
Figure 28.5 Transection of the gubernaculum at the level of the right internal inguinal ring. Continued dissection allows retraction of the testicle and its adnexa and affords optimal access to the inguinal rings. IAO, internal abdominal oblique; Gub, gubernaculum.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


