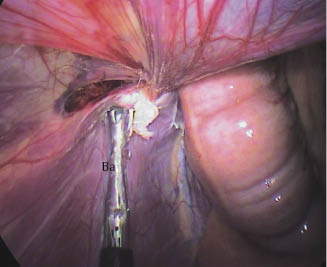
The vaginal ring is identified (Figure 15.2), and the mesorchium and the deferent duct are pulled caudomedially using a Babcock forceps introduced through the most ventral portal, and the sheath of a laparoscopic needle is introduced through the second portal. A flexible 150-cm-long, 2-mm-diameter polyethylene extension tube (Vygon) is introduced through the sheath, and the tip is positioned at the opening of the craniolateral part of the vaginal ring (Figure 15.3). The Babcock forceps is slightly displaced ventrally without releasing the mesorchium in order to press the visceral part of the vaginal ring onto its parietal part, 2 cm ventrally from its opening (Figure 15.4).

Figure 15.3 Right vaginal ring: injection of cyanoacrylate. Ba, Babcock forceps pulling the cord caudomedially; Ns, sheath of the laparoscopic needle; Ca, catheter; Co, spermatic cord.
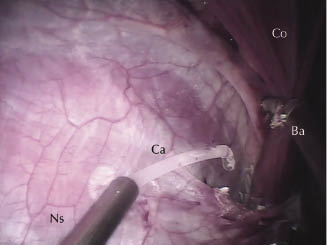
Figure 15.4 Right vaginal ring: The visceral part of the vaginal ring is pressed onto its parietal part, 2 cm ventrally from its opening using the Babcock forceps. Ba, Babcock forceps.
Then 2 mL of methyl-cyanoacrylate or n-butyl-2-cyano-acrylate are injected into the inguinal canal, including its margins, taking care to avoid the viscera, especially the bladder and the bowel. The lateral parts of the vaginal ring are compressed for 30 seconds using the Babcock forceps, taking special care not to get any glue on the forceps. Then the pressure exerted by the Babcock forceps is released and perfect closure of the vaginal ring with successful adhesion of its visceral and parietal parts is checked. The same procedure is performed on the right side. The abdomen is deflated and the skin portals are sutured in a routine manner.
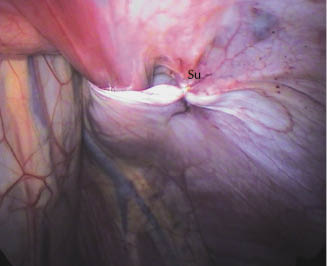
Alternatively, the lateral part of the left vaginal ring can be sutured prior to gluing using USP 0 lactomer (Polysorb with the Endo Stitch device, Covidien) or with the 3-0 V-Loc self-tying suture (Covidien) (Figure 15.5). Local anesthesia is then necessary and is performed using 2–3 mL of lidocaine. Cruciate stitches are used for both rings. This aims to reinforce the adhesive effect in very large rings.
Figure 15.5 Left vaginal ring. A cruciate stitch has been made on the craniolateral part using the 3-0 V-Loc self-tying suture (Covidien). Su, position of the suture.
Postoperative Management
Parenteral antibiotics are continued for 24 hours and anti-inflammatory drug treatment for 3 days. The horses can be discharged from the hospital 48 hours post-op. After 8 days of strict stall rest, the horse can be hand-walked twice daily for 2 weeks before returning progressively to training.
Conclusion
Procedure-Related Complications and Patient Outcome
Complications include all complications that can occur in standing laparoscopy, such as difficulties penetrating the abdomen, bleeding at the portal sites, organ puncture (spleen or hollow viscera), and technical problems in reaching the target tissue. Specific complications may include an inflammatory reaction after application of the cyanoacrylate, failure to fix the tissue, or glue application on other organs leading to adhesions.
Limitation of the Available Literature
Several laparoscopic herniorrhaphy or hernioplasty techniques have been described in horses to prevent inguinal herniation in stallions with quite good results according to the different authors, but a limited number of cases have been reported for most techniques (Fischer 2002). We have used the PFH technique in the recumbent (Rossignol et al. 2007) and the standing horse. Both techniques are described in other chapters. They require good technical skills and special laparoscopic instrumentation such as stapling devices, which are sometimes expensive. In our experience, some owners prefer to castrate the horse when it is not a breeding stallion for safety and/or economic reasons.
The technique described in this chapter can be performed with the horse standing and it requires no sophisticated instruments. It is a very straightforward procedure with few steps. The authors have operated on a small group of seven horses, including four normal horses and three horses with a history of inguinal hernias. All the horses were operated successfully. No preoperative or postoperative complications occurred. Vaginal rings were clearly visible and, before gluing, the space within the inguinal canal was clearly visible with the flank approach. This space enabled insertion of the Babcock forceps and the laparoscope, and could be enlarged by placing the mesorchium caudomedially.
Two milliliters of cyanoacrylate was sufficient to fix all rings. The mean surgery time was 25 minutes with more time required when combined suture was used and less time when gluing only was used.
Presuturing using either Endo Stitch or V-Loc self-tying suture was easily performed with no major difference between the two techniques.
There was no postoperative pain or swelling of the inguinal or the scrotal area.
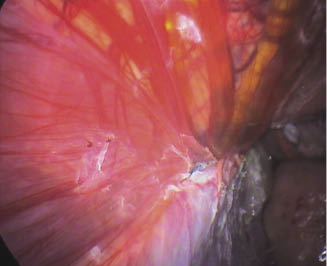
At the second laparoscopic evaluation performed in the first group, seven out of eight rings were fully closed with no room to insert any instrument into the inguinal canal (Figure 15.6). The ring where the glue was applied only on the margins was incompletely closed.
Figure 15.6 Right vaginal ring 3 weeks post-op after cyanoacrylate application alone. Note the full closure of the ring.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


