28 Horner’s syndrome
INITIAL PRESENTATION
Eye appears sunken or ‘disappears’ from view. Odd appearance to the animal’s face.
INTRODUCTION

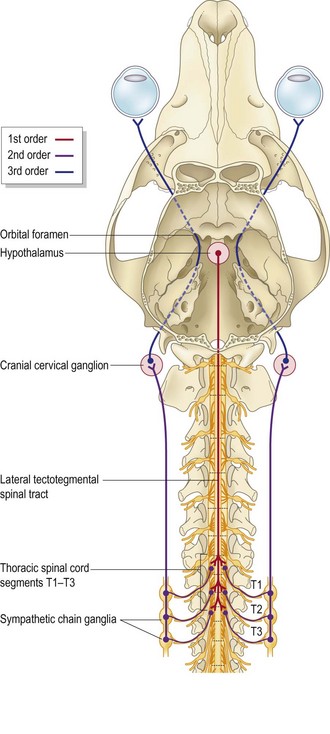
Pathway
Lesions of the oculosympathetic pathway (Fig. 28.2) can be categorized as first, second, or third order according to their anatomical site which can be most reliably discovered by finding concomitant neurological deficits. Pharmacological testing may help localize the lesion. It makes use of the phenomenon of denervation hypersensitivity which develops 8–10 days after a postganglionic lesion develops. A denervated receptor responds to a dilute concentration of neurotransmitter whereas a normal receptor would not. This may be helpful in differentiating second from third order lesions. thoracic radiography is used to investigate second order lesions.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


