Figure 33.2 The surgeon’s fingers are used (A) to bluntly enlarge an opening into the retroperitoneal space and to separate a kidney from the surrounding retroperitoneal fat, (B) to isolate the renal vasculature, and (C) to facilitate ligation of the renal vasculature.
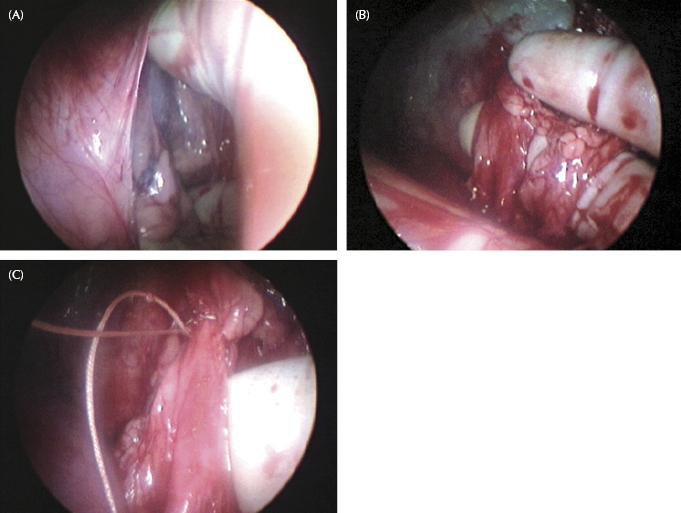
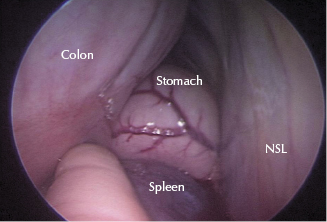
Figure 33.3 The surgeon’s hand is used to retract the colon from the nephrosplenic space to allow ablation of the nephrosplenic space. NSL, nephrosplenic ligament.
The disadvantage of having a hand in the abdomen is the larger incision required to access the abdomen than traditional laparoscopic procedures. Small flank incisions do have a tendency for incisional seroma, drainage, dehiscence, and infection. The lower aspect of the skin incision is left open to provide drainage and to prevent seroma formation. Long-term cosmetics for small flank incisions are generally very good, but in some cases, the orientation of the hair may change slightly or a small number of hairs may turn white.
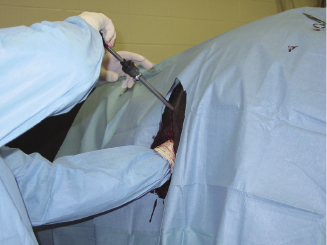
In equine surgery, HAL is becoming more popular and is the standard approach for certain procedures. The author commonly uses a standing hand-assisted laparoscopic approach for many procedures. The skin incision required for hand-assisted approaches is made in the middle of the paralumbar fossa and is started just ventral to the dorsal crus of the internal abdominal oblique muscle. The skin incision is generally 8–10 cm for most procedures. In standing procedures, a true grid or modified grid approach is used through the paralumbar musculature. Blunt dissection through the paralumbar musculature using the surgeon’s hand prevents inadvertent injury to the local vasculature. Using a plastic sterile sleeve also facilitates entry in and out of the flank incision. The peritoneum is bluntly penetrated using the surgeon’s fingers. Once the surgeon’s hand is within the abdomen, the laparoscope trocar-cannula unit is inserted through a separate skin incision dorsal to the paralumbar skin incision or through the flank musculature in the dorsal-most aspect of the paralumbar incision. The surgeon’s hand guards the peritoneum to prevent inadvertent injury to surrounding viscera as the trocar cannula is inserted (Figure 33.4). Handports can be used to provide a seal and to prevent loss of abdominal insufflation. In most cases, abdominal insufflation is not needed.
Figure 33.4 The surgeon’s hand guards the peritoneum to prevent inadvertent injury to surrounding viscera as the trocar cannula is inserted.
Hand-assisted laparoscopic ovariectomy is commonly performed for the removal of enlarged ovaries (Rodgerson et al. 2002; Goodin et al. 2011). Ovaries up to 40 cm in diameter have been removed using this approach. Hemostasis of the mesovarium is achieved using staple ligation, electrosurgical instrumentation, or a vessel-sealing device (LigaSure™). Ovaries are removed from the flank by either aspirating fluid or placing the transected ovary in a plastic bag. Once the ovary is within the plastic bag, it can be incised or transected to allow removal. The use of a tissue morcellator can also help in the removal of large ovaries.
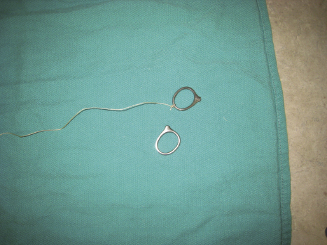
Nephrectomy in the adult horse is not commonly performed in equine surgery but can be easily and efficiently performed using a standing hand-assisted laparoscopic approach (Keoghan et al. 2003; Romero et al. 2010). Both left and right kidneys can be removed using a hand-assisted approach, and it is important to ensure the other kidney is functional prior to removal. Indications for nephrectomy in the horse include unilateral renal diseases, including hydronephrosis, nephrolithiasis, pyelonephritis, abscessation, neoplasia, nematodiasis, and ectopic ureter. In many cases, the affected kidney can be greatly enlarged, and the ability to bluntly and accurately dissect around the kidney is improved by having a hand within the abdomen. Isolation of the renal vasculature and the ureter is quite easy with a hand-assisted laparoscopic approach. The use of metal rings helps facilitate accurate ligation of the renal artery and vein (Figure 33.5) (Romero et al. 2010).
Figure 33.5 Metal ring attached to the suture for renal vascular ligation.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


