Chapter 106 Fractures and Dislocations of the Carpus
Injuries to the carpus occur most commonly as a result of trauma, and consist primarily of ligamentous injury resulting in hyperextension, subluxation, luxation, or fracture. Isolated fractures of the carpus are rare, and occur most commonly in racing greyhounds and working dogs.
Anatomy
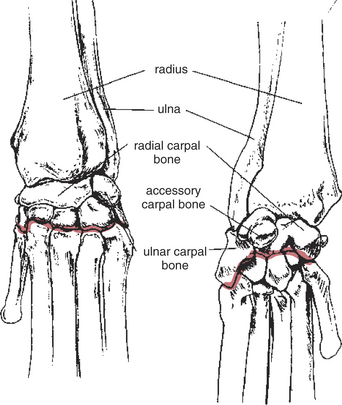
Osseous Structures (Fig. 106-1)
• The seven bones of the carpus are arranged in two rows; a small sesamoid bone in the tendon of insertion of the abductor pollicis longus is regionally associated with the carpal joint.
• The radial carpal bone is the largest of the carpal bones. It is located medially, and articulates with the radius proximally, and with the first, second, third, and fourth carpal bones distally.
• The ulnar carpal bone is the lateral bone of the proximal row. It articulates with the radius and ulna proximally, with the accessory carpal bone on its palmar aspect, and with the fourth carpal bone and fifth metacarpal bone distally.
• The accessory carpal bone is located on the palmar aspect of the lateral side of the proximal row. It articulates with the styloid process of the ulna proximally, and with the ulnar carpal bone.
• The distal row consists of the numbered carpal bones, the first (C1), second (C2), third (C3), and fourth (C4) carpal bones.
• C4 is the largest bone of the distal row, and articulates with the fourth and fifth metacarpal bones; the size of carpal bones C3 to C1 progressively decreases with the number of the bone.
Articulations
• The antebrachiocarpal joint is located between the distal radius and ulna, and the proximal row of carpal bones. It normally provides 70% of carpal range of motion.
• The middle carpal joint, between the proximal and distal rows of carpal bones, allows a small amount of flexion and extension, about 25% of carpal range of motion.
• The carpometacarpal joint, located between the distal row of carpal bones and the metacarpal bones, provides about 5% of carpal range of motion.
Ligamentous Structures
• Support to the carpus is provided by two superimposed sleeves of collagenous tissue, with tendons in between.
• The short radial collateral ligament has two parts, both of which originate from the styloid process of the radius; the straight part inserts on the medial part of the radial carpal bone and the oblique part inserts on the palmeromedial surface of the radial carpal bone.
• The short ulnar collateral ligament extends from the styloid process of the ulna to the ulnar carpal bone.
• The flexor retinaculum (transverse carpal ligament) provides support to the palmaro-proximal aspect of the carpus; it attaches laterally to the medial part of the accessory carpal bone and medially to the styloid process of the radius, the radial carpal bone and the first carpal bone.
• The palmar carpal fibrocartilage is quite thick and well defined; it crosses the palmar surface of the carpus and attaches to all of the bones except the accessory carpal bone. It also has strong attachments to the proximal aspect of the third, fourth, and fifth metacarpal bones.
• The accessory carpal bone is stabilized distally by two ligaments, which originate from its free end; one attaches to the fourth metacarpal bone (accessoro-metacarpal IV ligament) and the other to the fifth metacarpal bone (accessoro-metacarpal V ligament).
FRACTURES OF THE RADIAL CARPAL BONE
Preoperative Considerations
• Fractures of the radial carpal bone are rare and most commonly occur in working dogs during strenuous activity, resulting from jumps or falls.
• Chip fractures of the proximal dorsal border result from hyperextension of the radio-carpal joint.
• Moderate to severe lameness occurs immediately following the injury; however, in chronic cases only mild lameness, which resolves with rest, may be evident.
• Diagnosis requires a high index of suspicion since the majority of fractures are only minimally displaced.
Surgical Procedure
Technique
1. Place a tourniquet at the elbow and an Esmarch bandage from the nail bed to the proximal antebrachium.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


