Fractures
Small Splint Bones
Basic Information 
Epidemiology
Risk Factors
• Poor conformation, particularly at the carpus and tarsus, is a risk factor for proliferative periostitis of MC/MT-II and MC/MT-IV.
• Carpus or tarsus valgus or varus, and “offset knees” or “bench knees” exacerbate strains on these bones. Base narrow, toe-out conformation of the forelimbs may exacerbate the tendency for interference, specifically trauma to the contralateral MC-II.
Clinical Presentation
Disease Forms/Subtypes
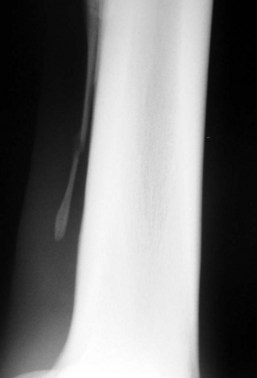
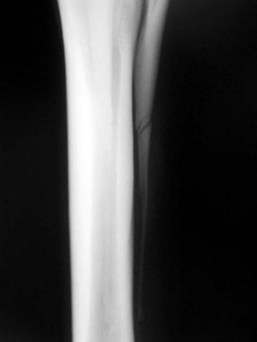
Splint bone fractures are divided into three types based on location: Proximal, mid-shaft, and distal (Figures 1 to 3).

History, Chief Complaint
• Horses with proliferative periostitis have a history of either gradual (insidious) or acute onset of lameness. Lameness may be unilateral or bilateral and is usually mild to moderate. Lameness improves with rest and antiinflammatory treatment and recurs with resumption of exercise. Sometimes a cosmetic blemish (focal hard swelling) is the first sign noted by the owner or trainer.
• Horses with splint bone fractures often have a history of external trauma (eg, a kick). Lameness in these cases is invariably acute and typically moderate to severe. Horses with fractures of the distal aspect that are associated with internal trauma (repetitive strain) and possibly a concurrent suspensory branch desmitis have a more variable history with onset being either acute or gradual and ranging from mild-to-moderate (rarely severe). Some distal splint fractures are discovered as incidental findings.
Physical Exam Findings
• A “splint” is recognized as a focal swelling along the shaft of the affected bone that is smooth and firm to hard on palpation. In some cases, the swelling is located axially, and the lesion can only be detected by palpation (most effectively with the limb held in flexion). Single lesions are most common, but multiple lesions affecting the same bone are sometimes present. Multiple lesions are most common on MC-II in young horses associated with early training. In this group, splints are also commonly bilateral. Horses exhibit variable degrees of pain on palpation of the splint. Pain is most severe in the acute stages and does not always correlate well with the degree of swelling or exostosis. Chronic splints, or those that have healed clinically, are typically not sensitive to palpation.
• Horses with distal splint bone fractures generally have very mild to moderate local soft tissue inflammation. The degree varies with the chronicity of the injury. Fractures that are more than 1 or 2 weeks old may have minimal residual associated swelling. Suspensory enlargement, most commonly of the associated branch, may also be present. Focal pain is common on firm palpation of the fracture site. If the fracture is chronic, a callus can often be palpated along with instability if the distal tip or “button” is pressed axially.
• Variable degrees of soft tissue swelling and pain on palpation of the fracture site are the hallmarks of fractures of the more proximal portions of the splint bones. Open wounds or abrasions may be present if the fracture is the result of external trauma. Signs of soft tissue infection are common with chronic fractures associated with open wounds.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


