Fig. 11.1
Distribution of rat liver lobes in terms of volume

Fig. 11.2
Portal vein anatomy of the rat liver
Fig. 11.3
Hepatic vein anatomy of the rat liver
The left lateral lobe represents approximately 30 % of the total liver volume. It is located in the left lateral position and is connected to the superior caudate lobe by interlobular ligaments. The narrow pedicle containing the vessels is attached to the infra-hepatic IVC and the base of the left portion of the median lobe.
The median lobe represents about 40 % of liver volume and consists of left (one third) and right (two thirds) portions separated by a deep fissure. It is located under the diaphragm and is fixed with the falciform ligament, which spans from the xyphoid and diaphragm to the liver forming the interlobular fissure. The median lobe has a wide base, surrounding almost half the circumference of the IVC.
The right liver lobe (20 % of liver volume) is located on the right side of the IVC and also consists of two distinct portions, an egg-shaped superior and a pyramid-shaped inferior lobe. The lobes are fixed dorsally with a hepatodiaphragmatic ligament to the diaphragm and ventrally towards the IVC.
The caudate lobe (7 % of liver volume) is located on the left side of the cava below the left lateral lobe; it is divided into two portions. The upper caudate lobe is connected to the left lateral lobe via a thin interlobular ligament and is fully covered by the lesser omentum, the lower caudate lobe is located behind the stomach in close proximity to the pancreas and spleen and is covered by a fibrous capsule, which is attached to the dorsal wall of the lesser omentum.
The paracaval liver portion (up to 3 % of the liver mass) does not represent a distinct anatomic unit, being the tissue at the dorsal parts of the bases of the right superior, right inferior, and caudate lobes, and covering the dorsal wall of the intrahepatic IVC, in addition to the liver tissue surrounding the main intrahepatic vessels which represents half of paracaval liver mass. This is the only liver tissue left in case of 97 % partial hepatectomy (PH).
Anatomical landmarks: [6] (Figs. 11.4, 11.5, 11.6).
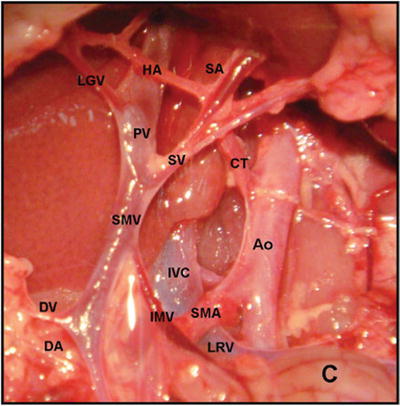


Fig. 11.5
Rat vascular anatomy from the upper abdomen (Source: [20]) Ao abdominal aorta, C colon, CT celiac trunk, DA duodenal artery, DV duodenal vein, HA hepatic artery, IMV inferior mesenteric vein, IVC inferior vena cava, LGV left gastric vein, LRV left renal vein, PV portal vein, SA splenic artery, SMA superior mesenteric artery, SMV superior mesenteric vein, SV splenic vein
Fig. 11.6
Anatomy of the liver hilum
There is no gallbladder in the rat .
The hepatic vein (HV) has no extra-hepatic margins for suture, therefore supra-hepatic IVC (SHIVC) to SHIVC reconstruction must be performed.
The esophagus is situated close to the liver, and the involvement of the esophagus at the total clamp of the SHIHC should be avoided.
Although the left median lobe is joined with the right median lobe, the predominant vessels of the left median lobe make a common channel with those of the left lateral lobe; this is important when preparing partial liver grafts.
Large communicating vessels between the PV and the para-esophageal vessels can be detected on the superior caudate lobe.
The right renal artery (RRA) is located behind the infra-hepatic IVC (IHIVC). The RRA usually branches into dual arteries, and the upper RRA branches into the right adrenal artery (Fig. 11.7).
The right adrenal vein and the lumbar vein flow directly into the IHIVC at the point of the lowest edge of the right inferior lobe; these veins occasionally make a common channel before the IHIVC (Fig. 11.7).
The left adrenal vein and the lower lumbar vein flow into the IHIVC at the junction of the left renal vein and the IHIVC (Fig. 11.7).
The common hepatic artery (CHA) is located posterior to the PV trunk, and the branched proper hepatic artery (PHA) and the gastro-duodenal artery (GDA) are located at the left side of the PV trunk; the PV trunk and these arteries are encased together by a thin sheath (Fig. 11.4).
11.3 Orthotopic Liver Transplantation
11.3.1 Donor Operation: The Liver Graft Procurement [21]
The procedure is performed under general intra-muscular anesthesia.
After the introduction of anesthesia, shave the abdominal wall using electric clippers and scrub the skin with povidone-iodine.
Make a midline xipho-pubic laparotomy incision, followed by a transverse incision. Retract the costal borders in a cranio-lateral direction to achieve the maximal liver exposure.
Moisten the bowels with warm saline and position them on the outside of the left abdominal cavity, covering with gauze. Frequent dripping of warm Ringer-Lactate (RL) onto the liver and bowels during laparotomy is recommended.
Divide the falciform, left triangular and gastro-hepatic ligaments; isolate and divide the left diaphragmatic vein between ligatures (Fig. 11.8).
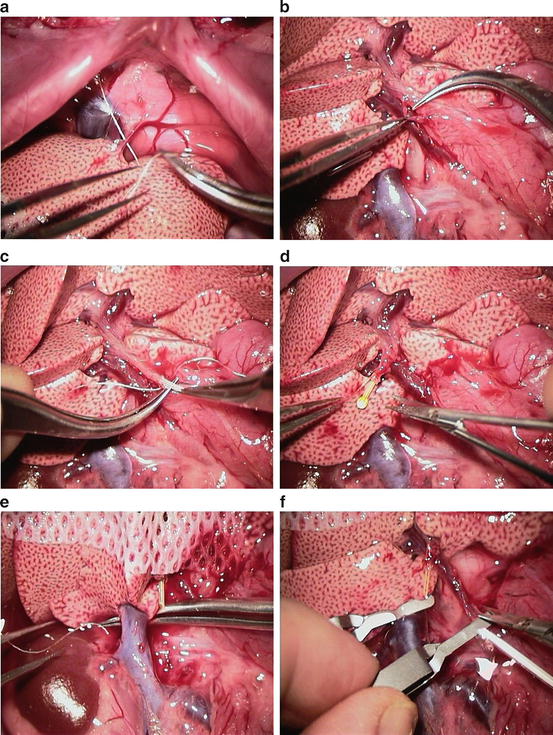
Fig. 11.8
Donor operation – liver graft procurement
Divide the hepato-esophageal ligament and vessels between ligatures or with electrocautery (Fig. 11.8a).
Divide the gastrosplenic vein.
Divide the proper hepatic artery between the ties (Fig. 11.8b)
Insert a 22G, 3.5 mm stent into the common bile duct through a small incision at approximately 1 cm distance from the hepatic hilum (Fig. 11.8c). Secure the stent in position with a 7–0 ligature (Fig. 11.8d).
Clean the PV by separating it from the surrounding tissues, hepatic artery and bile duct (Fig. 11.8d).
Isolate the IVC down to the left renal and right renal vein from surrounding tissues (Fig. 11.8e).
Divide the right suprarenal vein between the ligatures and free the liver from its posterior ligaments by cutting under gentle traction (Fig. 11.7).
Position a micro-clamp on the proximal part of the infra-hepatic IVC; this is needed to prevent bleeding after portal reperfusion during implantation (Fig. 11.8f).
Position a micro-clamp on the proximal part of the PV and cannulate it with a 21G needle as far as possible from the hilum and gently flush the liver with 20 ml of a cold preservation solution or RL (Fig. 11.8f). Concurrently, divide the supra-hepatic IVC to allow an adequate washout. Divide aorta in the chest to euthanise the animal. The liver cold perfusion should last between 1 and 2 min.
Cut the PV below at the level of cannula insertion (above the duodeno-pancreatic vein).
Cut the common bile duct distally to the ligature around the stent.
Cut the supra-hepatic IVC with a rim of the diaphragm; this tissue facilitates a safe supra hepatic IVC anastomosis during the implantation procedure.
Remove the liver graft and place it into a basin filled with cold RL and lay the basin on an ice pad.
Insert two Prolene 8–0 sutures at the opposite lateral edges of the supra-hepatic IVC.
Inspect all three vascular orifices to be anastomosed during the implantation procedure and ensure the vessel walls are clean.
Store the basin with the graft in the refrigerator at 0–4 °C.
11.3.2 The Recipient Procedure: The Orthotopic Liver Transplantation [21]
The transplantation procedure is performed under general inhalation anesthesia with isoflurane on a cone mask. At induction, use 3 % isoflurane to anesthetize the animal, then decreased to 2 % until the recipient hepatectomy is completed. For the anhepatic phase, pause the anesthesia and restart at 1–2 % after the liver graft is reperfused. Maintain the airflow at 1 L/min with 70 % FiO2 throughout the whole procedure.
Inject 10 ml of normal saline subcutaneously. Use antibiotic prophylaxis with 0.03 g of intramuscular piperacillin/tazobactam before laparotomy for procedures on immunosuppressed or immunocompromised animals.
After the introduction of anesthesia, shave the abdominal wall using electric clippers and prepared with povidone-iodine scrub. Place the animal on a warm pad for the procedure.
Perform a midline xipho-pubic laparotomy. Place retractors in latero-cranial and latero-caudal directions. Put a clamp on the xiphoid process and retract the rib cage cranially for adequate exposure. Check the breathing movements are not compromised by the retractor placements.
Moisten the bowels with warm saline, position on the outside of the left abdominal cavity, covering with gauze. Check for an adequate arterial blood supply and venous outflow. Frequent dripping of warm normal saline onto the liver and bowels during laparotomy is recommended.
Mobilize the liver as described in the liver procurement procedure (divide the liver ligaments, ligate and divide the left diaphragmatic vein, the hepato-esophageal vessels, the right suprarenal vein, the gastrosplenic vein and proper hepatic artery at the hilum)
Mobilize the bile duct and divide it at its confluence in the liver hilum
Isolate the IVC down to the left renal and right renal vein from surrounding tissues.
Mobilize the posterior part of the liver, isolate the supra-hepatic IVC and place a silk tie beyond it to enable an retraction on the vessel
Pause the inhalation anesthesia and continue ventilation with oxygen only.
Position a micro-clamp on the infra-hepatic IVC at the level of the right renal vein.
Position a micro-clamp on the PV at the level of gastrosplenic vein.
Commence timing the anhepatic phase of the procedure
Retract the supra-hepatic IVC in the caudal direction and place a Satinski clamp on the diaphragmatic rim around the vessel.
Divide the supra-hepatic IVC at the liver parenchyma border level.
Divide the portal vein in the liver hilum and the infra-hepatic IVC, both vessels just at the level of disappearing in the liver parenchyma.
Remove the liver and place the graft into the abdominal cavity.
Perform end-to-end supra-hepatic IVC anastomosis with a running 8–0 Prolene suture, fill the vessels with RL prior to finishing the anastomosis (Fig. 11.9).
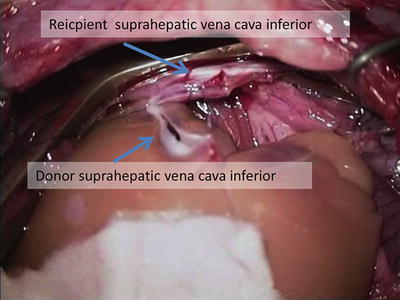
Fig. 11.9
End-to-end supra-hepatic IVC anastomosis
Anastomose the PV end-to-end with a running 9–0 Prolene suture (Fig. 11.10).

Fig. 11.10
Portal vein anastomosis, end-to-end
Infuse warm RL into the abdominal cavity to ensure the supra-hepatic IVC anastomosis is immersed and remove the micro-clamp from the PV (Fig. 11.11) and the Satinski clamp from the supra-hepatic IVC.
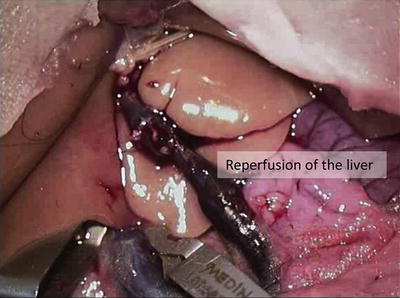
Fig. 11.11
Reperfusion of the liver graft after removing the clamps
Stop the timing of the anhepatic phase of the procedure, restart the inhalation anesthesia
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


