Endocarditis, Infective
Basic Information 
Clinical Presentation
Disease Forms/Subtypes
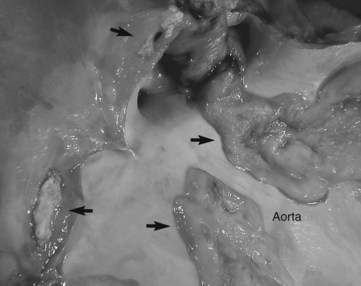
• Endocarditis can be categorized as acute, subacute, or chronic; bacterial or nonbacterial in origin; and valvular or mural (involving the endocardial walls), but most equine cases appear to be subacute or chronic and bacterial in origin and involve valvular structures (Figure 1).
• Rarely, parasitic infections may also result in endocarditis in horses.
• The left-sided valves (ie, mitral and aortic valve) are most frequently affected followed by the tricuspid and finally the pulmonic valve.
History, Chief Complaint
• Most frequent presenting complaints: fever and associated clinical signs (eg, anorexia, depression), although fever may be intermittent or even absent in some patients
• Signs of congestive heart failure, including tachypnea, coughing, edema, and complaints of severe exercise intolerance are possible
Physical Exam Findings
• Cardiac murmurs are heard in most patients, but endocarditis is not always accompanied by a detectable murmur, especially if nonvalvular structures are involved.
• Often, the endocardial lesions result in valvular regurgitation, but valvular stenosis may also occur.
• The classification of the murmur depends on the valves affected and whether a valvular regurgitation or stenosis is present. If the mitral or tricuspid valves are involved leading to regurgitation, a systolic murmur will be heard on either the left or right hemithorax. If the aortic valve is affected, often a diastolic murmur is heard because of valvular regurgitation. Valvular stenosis may also be a consequence of space-occupying lesions on the affected valves. In this case, a diastolic murmur may be ausculted over the tricuspid or mitral valves and a systolic murmur over the heart base if the aortic or pulmonic valve is stenotic.
• With heart failure, clinical signs such as tachycardia, tachypnea, coughing, harsh lung sounds caused by pulmonary edema, distension of the jugular veins, ventral pectoral or preputial edema, and weight loss may be encountered.
Etiology and Pathophysiology
• Occurs primarily in a subacute or chronic form and requires a complex interaction between endothelium, immune response, and circulating bacteria. After initial trauma to the endothelial cells and depositions of platelets and fibrin, a nonbacterial thrombotic lesion develops. During bacteremia, colonization with microorganisms occurs, creating a bacterial endocarditis visualized as a vegetative mass, leading to valvular regurgitations or stenosis and a cardiac murmur.
• Although a bacteremia is required, endocarditis may develop with no current or recent history of septic foci.
• The most frequently isolated bacteria are Staphylococcus spp., Streptococcus spp., Actinobacillus spp., Pasteurella spp., and Escherichia coli.
• Parasitic lesions caused by the nematode Strongylus vulgaris have also been reported (although rarely), primarily involving the aortic valves as well as the endothelium within the aorta and coronary arteries.
Diagnosis 
Differential Diagnosis
• Diagnosis is based on clinical findings of pyrexia, depression, weight loss, and possibly signs of heart failure and is supported by the presence of a cardiac murmur on auscultation. However, these signs are nonspecific and may reflect inflammation in any organ. An exact diagnosis is obtained by a positive blood culture result and echocardiographic examination showing vegetative lesions on the affected valves.
• Any disease resulting in systemic illness with fever, depression, and weight loss.
• Fibrotic and nodular thickening of the valves are incidentally visualized on echocardiography in horses. These structures generally have no inflammatory component but often result in a cardiac murmur. These findings can be difficult to differentiate echocardiographically from endocarditis lesions. However, these horses do not normally have clinical or hematologic signs of infection unless they have an infection in another organ system. When in doubt, diagnostic testing and treatment for endocarditis should be initiated.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


