CHAPTER 55 Dropsical Conditions Affecting Pregnancy
Hydrallantois and hydramnios, hydrops of the allantois and the amnion, respectively, are the two most common causes of dropsy of the fetal membranes and fetus in cattle. Other, less common causes include edema of the chorioallantois, fetal anasarca, and fetal edema with ascites and hydrothorax.1 In the largest published retrospective study of hydrops to date, Vandeplassche and associates documented that of a total of 60 cases, hydroallantois accounted for 88%, 5% of the cases were hydramnios, and 7% involved both compartments.2
HYDRALLANTOIS
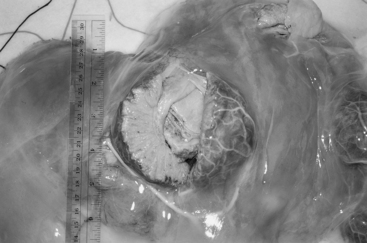
Hydrallantois is the single pathologic factor present in 85% to 90% of dropsical conditions in the bovine.1,2 Placental dysfunction is thought to be the cause of hydrallantois, although this condition is observed with both uterine and placental disease. Adventitious placentation commonly is present (Fig. 55-1), and the number of caruncles also may be deficient. This deficiency may be due to a congenital lack of development or to uterine disease acquired later in life. A reduction in the number of caruncles also has been noted with hydrallantois, and those that are present tend to be hypertrophied.3 The condition is seen sporadically in both dairy and beef cows, and dams carrying multiple fetuses are at greater risk for hydrallantois. An increased prevalence of hydrallantois has been noted in recipient cattle carrying fetuses produced by in vitro fertilization and by transgenic and cloning technologies.4,5
The structural and functional changes in the chorioallantois that lead to hydrallantois result in the excessive production of a transudative fluid that resembles plasma.1 In severe hydrallantois, the accumulated fluid volume may reach 150 to 250 L, and the combined weight of the dropsical fluids, membranes, and fetus can exceed 225 kg.3 Fluid composition studies comparing allantoic fluid from normal cows in late gestation and from those suffering from hydrallantois have demonstrated marked differences in sodium, potassium, chloride, and creatinine levels.2,6,7 In hydrallantois, the levels of these electrolytes are much higher, more closely resembling plasma levels.8 In addition, lower peripheral plasma concentrations of estradiol have been observed in cows suffering from hydrallantois.7 The exact role of estrogen deficiency in the maintenance of fetal membrane permeability and its effect on allantoic and amniotic fluid volume in the cow remains uncertain. Studies in pigs and ovariectomized sheep, however, point to a link between the estrogen-to-progesterone ratio and fetal fluid volume.8,9
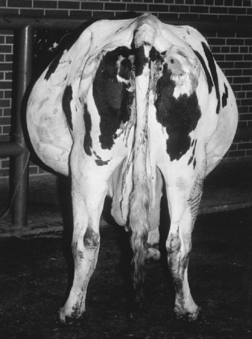
The clinical signs associated with hydrallantois vary with the volume of fluid at presentation. Abdominal distention rarely has been noted as early as the fifth month of gestation.3 The typical case of hydrallantois, however, is characterized by a larger than normal accumulation of allantoic fluid during a 5- to 20-day period in the last trimester of pregnancy3 (Fig. 55-2). Mild cases may remain undiagnosed or may be suspected only at parturition when an abnormally large volume of fetal fluids is expelled. In such instances, the producer may have assumed that the dam was carrying twins. In the more severe cases, progressive abdominal distention during the last 4 to 6 weeks of pregnancy worsens to such an extent as to decrease appetite and cause difficulty moving or rising.10 Progressive maternal tachycardia, anxiety, reduced appetite, and dehydration should be anticipated with untreated hydrallantois. Recumbency and metabolic problems, particularly ketosis, are therefore potential complications associated with advanced cases of hydrallantois, and these will be even more likely should the condition be associated with multiple fetuses. The combined weight of the fetus(es) and allantoic fluid also may result in either prepubic tendon rupture or secondary ventral abdominal muscle herniation.
HYDRAMNIOS
Hydramnios causes approximately 10% of the cases of hydrops of the fetal membranes in cows.1 The condition is characterized by gradual accumulation of excessive amniotic fluid, with progressive abdominal enlargement in the dam during the last trimester of pregnancy. The abdominal distention typically is slower to develop than in hydrallantois.3 Hydrops of the amnion usually is the result of an abnormal fetus and is therefore considered a fetal problem, whereas hydrallantois is due to maternal abnormalities of placentation. From midgestation to term, amniotic fluid normally is swallowed or inhaled into the large bronchi of the fetus and subsequently absorbed.11 Hydramnios results from fetal abnormalities that prevent swallowing or intestinal transport of amniotic fluids.1 During late gestation, the volume of normal amniotic fluid reaches between 3.8 and 7.6 L; however, in hydramnios, the volume will increase to 19 to 114 L. The fluid is viscous and syrupy in consistency.1
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


