Chapter 83 Disorders of Micturition
Micturition involves the passive storage and the active voiding of urine. Processes that interfere with the storage and voiding of urine are termed micturition disorders. The loss of voluntary control of micturition is defined as urinary incontinence.
NORMAL ANATOMY AND PHYSIOLOGY OF THE URINARY BLADDER
Nervous Control
Higher Centers of Innervation
For voluntary control of micturition to occur there must be integration among the cerebral cortex, the pons, and the spinoreticular tract. A second pathway from the cerebral cortex to the sacral nuclei coordinates voluntary sphincter control. In addition, cerebellar neurons inhibit nervous transmission to the reticulospinal pathways in the pons.
ETIOLOGY OF MICTURITION DISORDERS AND INCONTINENCE
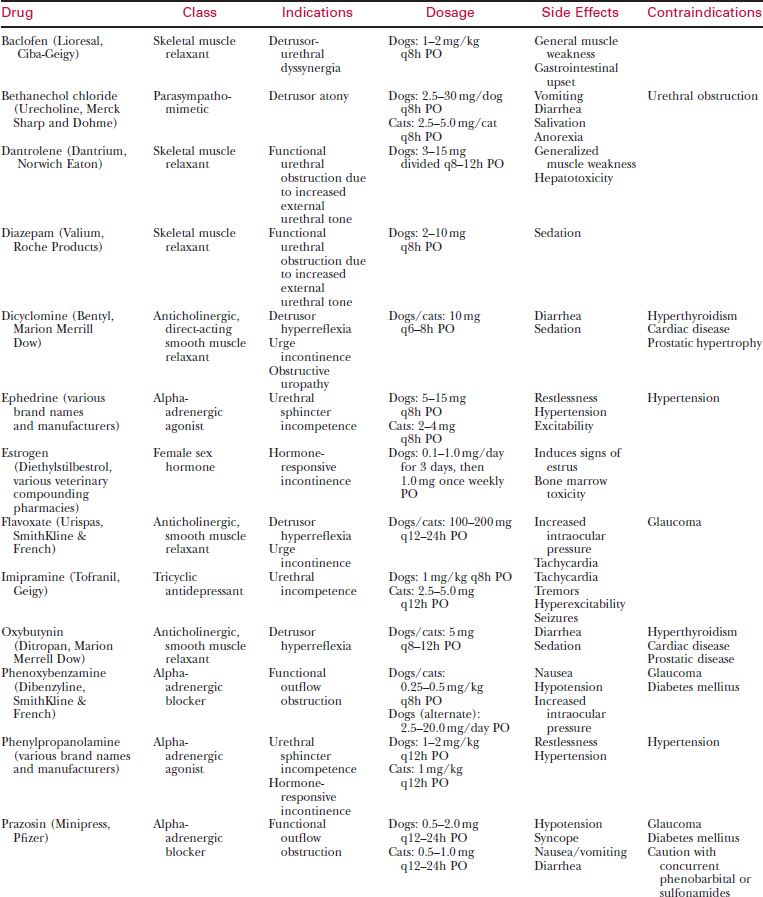
Disorders of micturition and continence can be divided broadly into two types: neurogenic and non-neurogenic (Table 83-1).
Table 83-1 DISORDERS OF MICTURITION
| Type of Disorder | Clinical Signs | Treatment |
|---|---|---|
| Neurogenic | ||
| Lower motor neuron bladder | Distended, easily expressed | No effective therapy, |
| Continuous incontinence | Manual expression 3–4 times daily | |
| No perineal or bulbospongiosus reflex | Trial with bethanechol chloride | |
| No detrusor reflex | Concurrent antibiotics | |
| Upper motor neuron bladder | Large, firm bladder | Aseptic intermittent catheterization |
| Difficult manual expression initially | Concurrent antibiotics | |
| Increased sphincter tone ± detrusor reflex | Antispasmodics or smooth muscle relaxants | |
| Long-term management usually frustrating | ||
| Detrusor-urethral dyssynergia | Large, non-expressible bladder | Prazosin |
| Initiation of urine stream with abrupt disruption of urination | Other alpha-antagonists | |
| Baclofen | ||
| Intact spinal reflexes | Diazepam | |
| Bladder easily catheterized | Dantrolene | |
| Non-neurogenic | ||
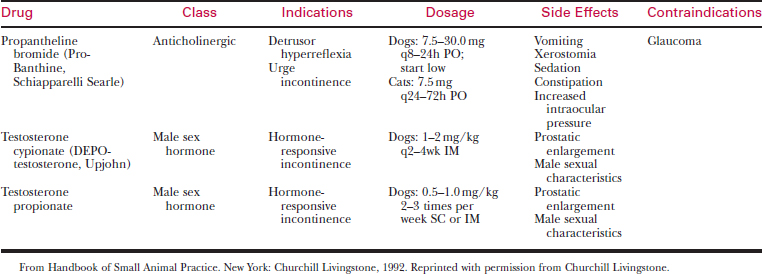
| Hormone-responsive incontinence | Older, neutered animal | Diethylstilbestrol (females) |
| Voluntary control of urination with intermittent incontinence | Testosterone (males) | |
| Phenylpropanolamine | ||
| Incontinence usually when relaxed or asleep | ||
| Urethral incompetence (stress incontinence) | Loss of voluntary control when placed in a stressful situation or at rest | Phenylpropanolamine |
| Imipramine | ||
| Ability to urinate voluntarily | ||
| Urge incontinence (detrusor hyperreflexia) | Frequent small urinations | Flavoxate |
| Hyperreflexive detrusor | Oxybutynin | |
| Urine spraying | Dicyclomine | |
| Stranguria | Propantheline bromide | |
| Overdistension atony | Large flaccid bladder | Remove mechanical obstruction |
| Continuous incontinence | Indwelling bladder catheterization | |
| Large residual urine volume | Bethanechol chloride | |
| Intact perineal and bulbospongiosus reflex | ||
| No detrusor reflex | ||
| Paradoxical incontinence | Stranguria | Remove obstruction |
| Persistent urine dribbling | Indwelling catheterization | |
| Large, turgid bladder that is difficult to express | Surgical exploration | |
| Cystoscopy | ||
| Ectopic ureter(s) | Continuous or intermittent dribbling of urine | Surgery |
| Ability to urinate voluntarily | Phenylpropanolamine | |
| Pelvic bladder | Loss of voluntary control when placed in a stressful situation or at rest | Phenylpropanolamine |
| Surgery | ||
| Ability to urinate voluntarily | ||
Neurogenic Disorders
Lower Motor Neuron Bladder
Lower motor neuron, or atonic, bladder results from lesions involving the sacral spinal cord segments or pelvic nerve, including intervertebral disc disease, cauda equina syndrome, sacroiliac luxations, sacrococcygeal fracture or separation, and tumors (e.g., spinal lymphoma). This type of disorder causes both detrusor and sphincter areflexia. Dribbling of urine with the bladder remaining full is often referred to as overflow incontinence.



