38 Diseases of the Stomach
The clinical signs and signalment are often clue enough to establish a tentative diagnosis of GDV, though this needs to be differentiated from a case of simple dilation. This can be done with radiographs (Fig. 38-1) and the pylorus dorsal to the body of the stomach, though in compromised animals it may be prudent to stabilize the dog before radiography. Right lateral is the preferred view to use for diagnosis. Check the radiographs carefully for evidence of free air; this could indicate gastric rupture.
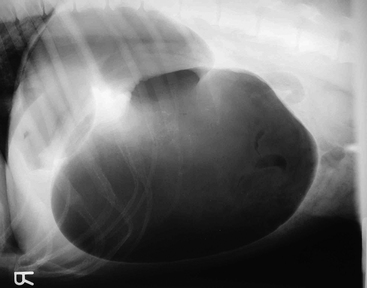
Figure 38-1 Lateral radiograph showing gas distention of the stomach with compartmentalization (double bubble).
Routine blood work and urinalysis are indicated to rule out concurrent illnesses and to assess for the severity of acid-base and electrolyte abnormalities. Lactate analysis is also helpful. Markedly elevated lactate concentrations are associated with a poorer outcome. Blood pressure should be monitored to assess for efficacy of resuscitation efforts. An electrocardiogram is also recommended. Most arrhythmias develop during anesthesia or postoperatively and do not appear to correlate to outcome. Arrhythmias at presentation do seem, however, to be associated with increased mortality.
< div class='tao-gold-member'>



