Chapter 67 Diseases of the Stomach
VOMITING
Vomiting is a common clinical sign associated with many gastrointestinal (GI) and non-gastrointestinal (non-GI) disorders of dogs and cats. Vomiting is a central nervous system reflex that is integrated in the vomiting center of the brain stem. Afferent stimuli can originate from the cerebral cortex, chemoreceptor trigger zone, pharynx, peritoneum, or abdominal viscera. Vomiting must be differentiated from regurgitation, which is the passive expulsion of undigested food indicating a pharyngeal (swallowing) or esophageal disorder (see Chapter 65).
Etiology
Vomiting is a clinical sign, rather than a diagnosis, and can be associated with numerous GI and non-GI disorders (Table 67-1).
Clinical Signs
Diagnosis
The diagnostic approach to vomiting is directed toward identifying the underlying disorder (see Table 67-1) and is influenced by whether vomiting is acute or chronic and by the associated historical and physical findings.
Table 67-1 CAUSES OF VOMITING IN DOGS AND CATS
| Acute Vomiting (<1wk) | Chronic Vomiting (>1–2wk) |
|---|---|
CNS, central nervous system; NSAIDs, nonsteroidal anti-inflammatory drugs.
Acute Vomiting
Acute vomiting is a common problem in dogs and cats and may be caused by benign, self-limiting disorders such as acute gastritis or serious life-threatening diseases such as acute pancreatitis, intestinal obstruction, or acute renal or hepatic failure (see Table 67-1).
Physical Examination
Laboratory Evaluation
When further diagnostic testing is indicated, a stepwise strategy is recommended.
Radiography
Endoscopy
Treatment
Treatment strategies in the vomiting animal are directed toward the following:
Fluid Therapy
Dietary Management of Acute Vomiting
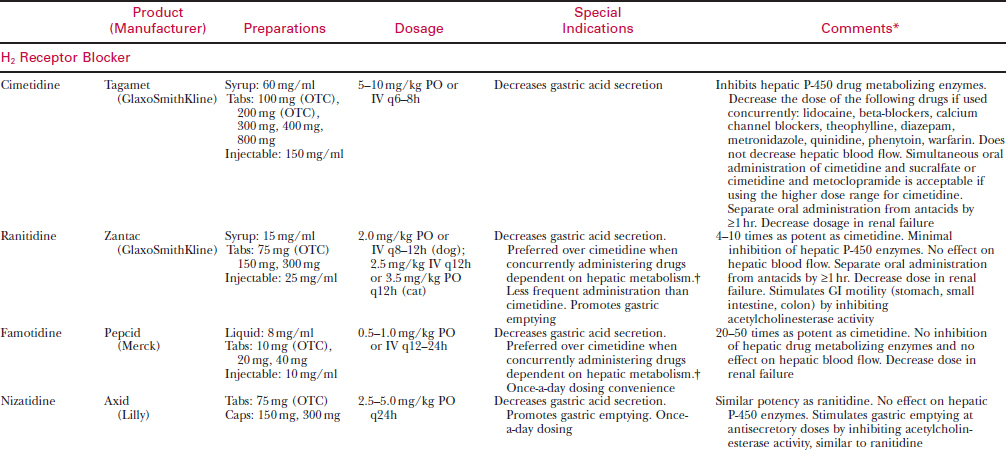
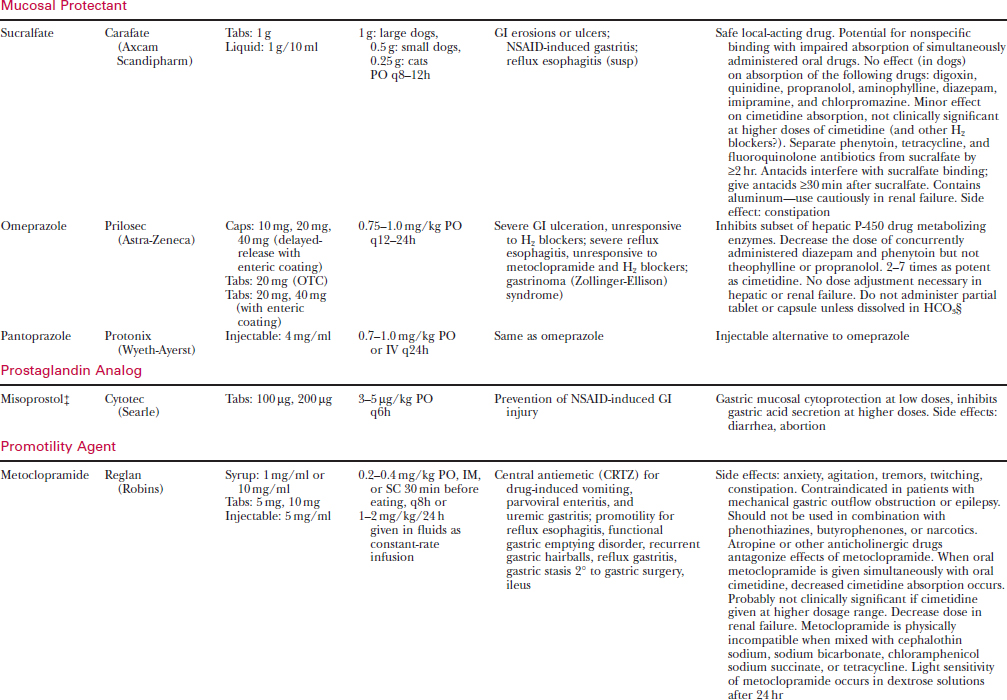
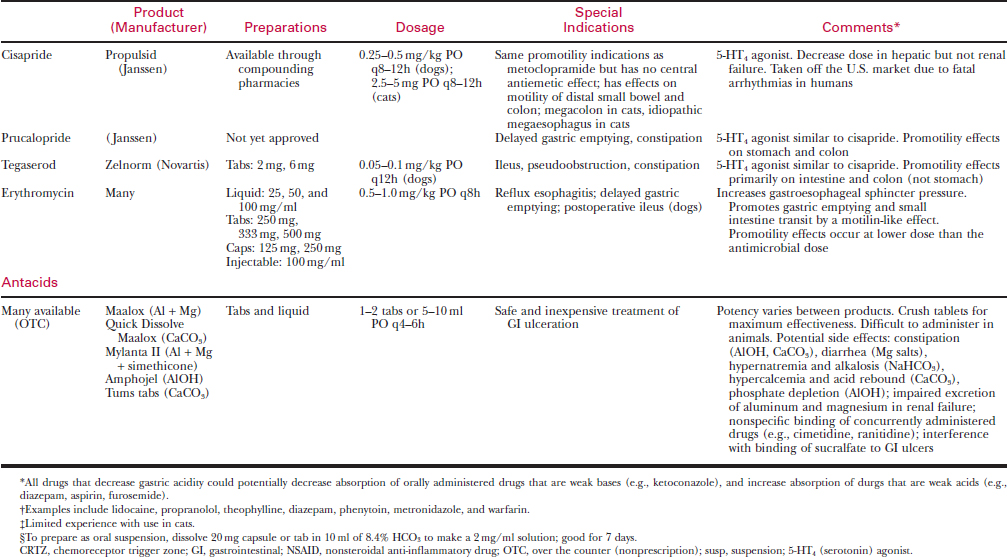
Antiemetics
Phenothiazines
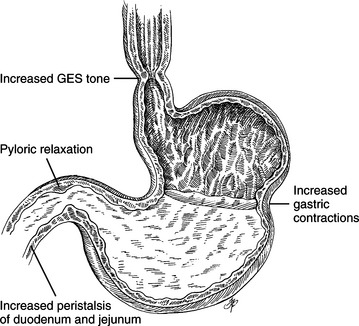
Metoclopramide
Serotonin Antagonists
Butorphanol
Anticholinergic Drugs
ACUTE GASTRITIS
Etiology
There are numerous potential etiologies of acute gastritis (see Table 67-1), but the cause often is not determined. Possible causes include the following:
Diagnosis
Physical Examination
The physical examination is usually unremarkable except for dehydration in severe cases.
Dietary Restriction
Maintenance of Hydration
GASTRIC FOREIGN BODIES
Etiology
Clinical Signs
Diagnosis
Physical Examination
This is often unremarkable except when gastric foreign bodies are very large and palpable.
Treatment
Endoscopic Removal
Preparation
Procedure
Gastrotomy
If endoscopic equipment is unavailable or the object cannot be retrieved endoscopically, gastrotomy is indicated (see Chapter 68).
GASTRODUODENAL ULCERATION
Etiology
Many disorders have been associated with gastroduodenal ulceration (Table 67-2). Ulceration is more likely when two or more risk factors are present. General mechanisms of gastroduodenal ulceration include direct damage to the gastric mucosal barrier, increased gastric acid secretion, delayed gastric epithelial renewal, and decreased gastric mucosal blood flow.
Table 67-2 RISK FACTORS FOR GASTRODUODENAL ULCERATION
Nonsteroidal Anti-Inflammatory Drugs
Nonsteroidal anti-inflammatory drugs (NSAIDs) (see Table 67-2) are frequent causes of gastric ulceration. These drugs inhibit prostaglandin synthesis, which decreases mucosal blood flow and alters gastric mucus production, thus predisposing to ulceration. Dogs are more susceptible to the ulcerogenic effects of NSAIDs than are humans.
Glucocorticoids
Glucocorticoid therapy has been associated with gastric erosions and bleeding but usually only when combined with other risk factors for ulceration such as NSAIDs or in dogs with spinal cord disease (see Table 67-2). Dexamethasone, especially at high doses, is more likely to cause GI bleeding than is prednisolone.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


