Chapter 8 Diseases of the Nervous System
The nervous system can be divided into two primary divisions: the central nervous system (CNS), composed of the brain and the spinal cord, and the peripheral nervous system (PNS), composed of the cranial nerves and the peripheral nerves that connect the outside sensory world to the brain.
BRAIN
Trauma
DIAGNOSIS
Table 8-1 Clinical Rating Scale for Evaluation of Craniocerebral Trauma
| Criteria | Score* |
|---|---|
| Motor activity | |
| Normal gait, normal reflexes | 6 |
| Hemiparesis, tetraparesis, or decorticate activity | 5 |
| Recumbent with intermittent extensor rigidity | 4 |
| Recumbent with constant extensor rigidity | 3 |
| Recumbent with intermittent extensor rigidity/opisthotonos | 2 |
| Recumbent, hypotonic with depressed-absent spinal reflexes | 1 |
| Brainstem reflexes | |
| Normal PLR and OVRs | 6 |
| Slow PLR and normal to reduced OVRs | 5 |
| Bilateral/unresponsive miosis and normal-to-reduced OVRs | 4 |
| Pinpoint pupils and reduced-to-absent OVRs | 3 |
| Unilateral/unresponsive mydriasis and reduced-to-absent OVRs | 2 |
| Bilateral/unresponsive mydriasis and reduced-to-absent OVRs | 1 |
| Level of consciousness | |
| Occasionally alert and responsive | 6 |
| Depressed/delirious, but capable of response to stimulus | 5 |
| Obtunded/stupor, but responds to visual stimuli | 4 |
| Obtunded/stupor, but responds to auditory stimuli | 3 |
| Obtunded/stupor, but responds to noxious stimuli | 2 |
| Comatose and unresponsive to noxious stimuli | 1 |
* Prognosis: grave for 3-8 total score; poor to guarded for 9-14 total score; and good for 15-18 total score. PLR, pupillary light reflex; OVR, oculovestibular reflex.
From Fenner WR: Diseases of the brain. In Ettinger SJ, Feldman EC, editors: Textbook of veterinary internal medicine, ed 5, Philadelphia, 2000, WB Saunders, by permission.
TREATMENT
Neoplasia
DIAGNOSIS
Blood work: complete blood cell count (CBC) and serum chemistries
TREATMENT
Treatment of the tumor
Idiopathic Epilepsy
Idiopathic epilepsy is predominantly a disease in German shepherds, miniature and toy poodles, Saint Bernards, cocker spaniels, beagles, Irish setters, golden retrievers, and some mixed breeds. Seizures usually begin between 1 and 3 years of age. Affected animals may exhibit a short aura during which the animal may act abnormally. They may hide, seek companionship, vocalize, or exhibit other abnormal behaviors. Seizures are usually generalized in nature, lasting anywhere from 1 to 2 minutes. After the seizure, the animal is usually disoriented and occasionally blind. Seizures may occur singly or in clusters and may reoccur at fairly regular intervals. In some animals, inciting events such as excitement or estrus have been shown to precipitate seizure activity. Although the cause of idiopathic epilepsy is unknown, a hereditary basis has been suggested.
DIAGNOSIS
Status Epilepticus
TREATMENT
Immediate treatment
SPINAL CORD
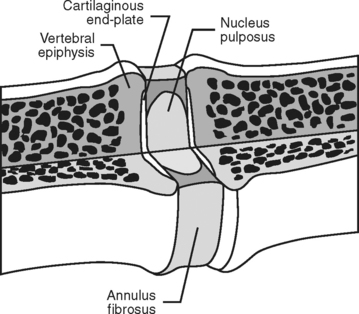
Just like the brain, the spinal cord is protected by a bony housing, the vertebral column. The spinal cord is located within the spinal canal, dorsal to the vertebral bodies. Between each of the vertebral bodies is a cushion known as the intervertebral disk. These disks are composed of an outer fibrous layer, the annulus fibrosus, and an inner gel-like nucleus, the nucleus pulposus. Their presence allows a larger range of motion in the vertebral column and prevents the vertebral bodies from rubbing against each other (Fig. 8-1).
Intervertebral Disk Disease
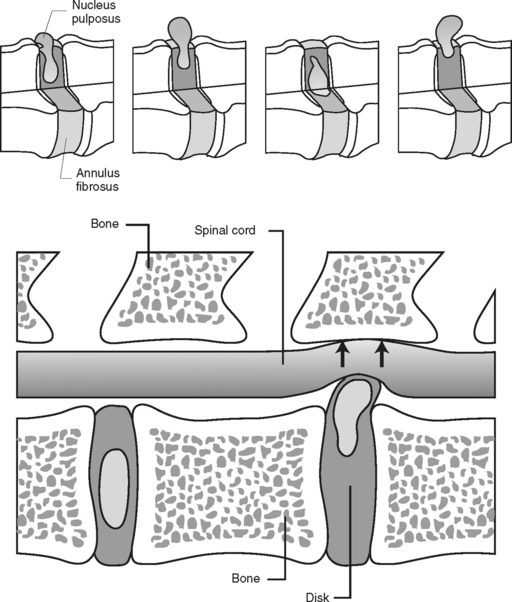
By far, one of the most common disorders involving the spinal cord of small animals is intervertebral disk disease. Disk protrusions can occur in all breeds of dog and occasionally in cats. It has been reported that 75% to 100% of all disks in chondrodystrophic breeds have undergone degenerative changes by 1 year of age. Disk protrusion or extrusion occurs most commonly in the cervical, caudal thoracic, and lumbar spine. Two types of herniations have been reported. Type 1 (common in younger dogs) involves acute rupture of the annulus fibrosus and extrusion of the nucleus pulposus up into the spinal canal. In type 2 herniation (common in older [>5 years] large-breed dogs) the extrusion occurs over a longer period, producing less acute and less severe clinical signs. The severity of spinal cord injury depends on the speed at which the disk material is deposited into the spinal canal, the degree of compression, and the duration of compression. Clinical signs may be related to the location of the lesion (Fig. 8-2).
DIAGNOSIS
TREATMENT
Type 1
Spinal Cord Trauma
Acute spinal cord injuries of the dog and cat usually result from motor vehicle accidents, gunshot wounds, or fights. The spinal cord trauma is sudden in onset and may be related to the velocity of cord compression, the degree of compression, and the duration of the compressive force. Signs of injury are typically nonprogressive, although they may worsen over the first 48 hours before stabilization. Injury may occur at a single or multiple levels within the spinal cord.



