CHAPTER 20Cervical Tears
Cervical lacerations or tears, which often form defects when healed, have long been recognized as a cause of mare infertility. The cervix can function as a physical barrier, separating the uterus from the vagina. During pregnancy and diestrus, when under the influence of progesterone, this muscular tube is tightly closed. This barrier protects the uterus from infectious agents and debris that may have gained access to the cranial vagina. Depending on size, a defect in the cervix may adversely affect cervical function and thus the ability of the mare to conceive and carry a foal to term. It is important for fertility that cervical defects be promptly recognized and managed appropriately.
ANATOMIC FEATURES OF THE EQUINE CERVIX
The cervix of a nongravid mare in diestrus typically is a strong and resilient tubular smooth muscle sphincter measuring 2.5 to 5.0 cm in diameter and 5.0 to 7.5 cm in length.1 The muscular cervix is an extension of the uterine body, with the distal portion protruding caudally into the anterior vagina and containing the external cervical os. The endometrial folds of the uterine body continue longitudinally along the length of the cervical canal and create the folded mucosal surface of the cervical lumen. The cervical epithelium is made up of ciliated epithelial and mucus-producing cells.2 The vascular and nerve supply to the cervix comes primarily from the vaginal artery, vein, and nerve. The vaginal artery arises from the internal pudendal artery, branching from the internal iliac artery, which is a terminal branch of the abdominal aorta.3
ETIOLOGY OF CERVICAL LACERATIONS
An important characteristic of the equine cervix is the inherent elasticity of the cervical tissue. This elasticity allows the cervical walls to expand greatly for passage of the fetus during parturition. Cervical lacerations occur most commonly from excessive and/or abrupt cervical stretching during foaling. This is especially true if the cervix has not relaxed sufficiently. Cervical tears are more likely to occur during dystocia than during normal parturition. Nevertheless, a cervical tear can occur during unassisted, normal foaling. In fact, one study showed that 86% of the mares presented for cervical defect repair sustained the injury after an apparently normal foaling.4 Manipulations performed to deliver a fetus vaginally from a mare in dystocia, are sometimes done with swollen tissues and inadequate lubrication.5,6 This places the cervix at increased risk for injury. A fetotomy also increases the risk for cervical trauma.
Other causes of cervical defects are rare. Cervical laceration in an Arabian mare as a result of cervical penetration by the stallion’s penis during breeding has been reported.7 Cervical incompetency due to congenital failure of cervical closure has been reported in a 2-year-old filly.8
No site around the circumference of the cervix has been reported to be predisposed to tearing.9 This finding is supported by our clinical experience. Presentation for cervical defect repair in the thoroughbred is most commonly done in the middle-aged, multiparous mare.4
DIAGNOSTICS
Careful examination of the cervix is an important part of the reproductive examination of the mare. A vaginal speculum is routinely used in evaluation of the cervix. Cervical defects can be overlooked, however, on the basis of visual inspection alone. This is especially true during the estrous period, when visualization of the defect may be obstructed because of the presence of tissue edema. Edematous cervical folds may overlap and obscure the laceration site from view.7 The cervix ideally is examined with the mare in diestrus. The cervix exhibits minimal edema and is contracted and tight, allowing accurate evaluation of the competency of the cervical wall. Digital palpation is necessary for full appreciation of a cervical defect.
Recording or describing the site of a cervical abnormality is simplified by considering the external margin of the cervix as analogous to the face of a circular clock (Fig. 20-1). The most dorsal aspect of the cervix corresponds to the 12 o’clock position, whereas the ventralmost aspect corresponds to the 6 o’clock position. Palpation of the cervix is done using a sterile glove or sleeve and an ample amount of sterile lubricant. The cervical wall is evaluated between the operator’s thumb and index finger, with either the thumb or finger inserted into the lumen. The circumference of the cervix is carefully palpated to identify any defect in the cervical wall. The clock face analogy is used to characterize the location of the defect (Fig. 20-2).
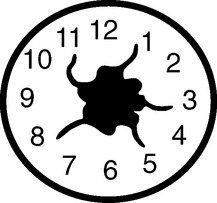

Figure 20-2 A cervical laceration is visible extending from the 4 o’clock to the 6 o’clock position.



