Chapter 7 Case Management
CANINE “HIT-BY-CAR” LIMB FRACTURE
Preanesthesia
▪ With regard to blood work, at a minimum, packed cell volume (PCV), total protein (TP), blood glucose, and blood urea nitrogen (BUN) should be measured
▪ Anemia secondary to hemorrhage must be corrected before anesthesia; any patient with PCV < 20% should receive blood transfusion
▪ Perform electrocardiography (ECG); any bodily trauma may produce myocardial injury and result in traumatic myocarditis that manifests as ventricular arrhythmias (premature ventricular contractions or ventricular tachycardia)
▪ An intravenous (IV) catheter is placed for the administration of anesthetic agents and resuscitation fluids; patients in shock are administered “shock-dose” fluids at 90 ml/kg IV; in addition, hypertonic saline or colloids may be administered
Induction
▪ Propofol may induce respiratory depression; use with caution in patients with respiratory trauma; give half the calculated induction dose over 60 seconds; preoxygenate (with oxygen administered via face mask for 5 minutes) before induction to prevent hypoxemia
▪ Ketamine and benzodiazepine induction may lead to tachycardia or arrhythmias and should be avoided in patients with cardiac trauma; use is recommended in patients with respiratory disease or with pneumothorax, as ventilation is minimally depressed
▪ Opiate and benzodiazepine induction may lead to hypoventilation or apnea; use with caution in patients with respiratory trauma; bradycardia may result and can be prevented or treated with anticholinergic agents
▪ Inhalant induction by face mask is acceptable only if patient is not vomiting and pneumothorax is not present
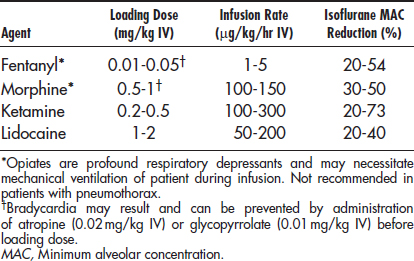
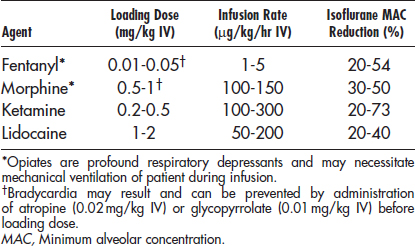
Analgesia
▪ Epidural administration if fracture present in forelimb or hindlimb; if performed before surgery, decreases inhalant requirement during surgery and provides postoperative analgesia for up to 24 hours (if preservative-free morphine is used)
▪ Fentanyl patch placement before surgery (blood levels of fentanyl and therefore analgesia are not present for 8 to 12 hours after placement; provides only postoperative analgesia)
Maintenance
▪ Isoflurane and sevoflurane are preferred over halothane; halothane sensitizes myocardium to catecholamine-induced arrhythmias (exercise caution in patients with traumatic myocarditis)
Monitoring
▪ ECG: watch for arrhythmias (particularly ventricular premature contractions [PVCs] and ventricular tachycardia)
▪ Blood pressure should be monitored; mean arterial pressure (MAP) should be maintained above 60 mm Hg and systolic arterial pressure (SAP) above 90 mm Hg
□ Hypotension = MAP < 60 mm Hg, SAP < 90 mm Hg
• Replace surgical blood loss at 1:3 ratio—for every milliliter of blood lost during surgery, 3 ml of crystalloid (e.g., lactated Ringer’s solution [LRS]) is administered IV
• Hemorrhage resulting in PCV < 20% requires blood transfusion or hemoglobin-substitute administration
CANINE OPHTHALMIC SURGERY
Preanesthesia
Agents (mg/kg IM; use half if administering IV)
Oxymorphone* 0.5-0.2 + acepromazine 0.02-0.05 ± glycopyrrolate 0.01
Morphine* 0.5-1 + acepromazine 0.02-0.05 ± glycopyrrolate 0.01
Buprenorphine 0.01-0.02 + acepromazine 0.02-0.05 ± glycopyrrolate 0.01
Midazolam† (or diazepam) 0.1-0.3 can be substituted as a sedative
Induction
▪ Ketamine and benzodiazepine induction may lead to increased intraocular pressure and is not recommended
▪ Opiate and benzodiazepine induction has no direct effect on intraocular pressure but may lead to hypoventilation or apnea, which indirectly increases intraocular pressure
Neuromuscular Blockade
▪ Mechanical ventilation is necessary; set tidal volume to 10 to 20 ml/kg, respiratory rate to 6 to 12 breaths per minute, and peak inspiratory pressure to < 20 cm Hg
Nondepolarizing Neuromuscular Blocking Agents
| Agent | Initial Dose (mg/kg IV) | Repeat Dose (mg/kg IV) |
|---|---|---|
| Atracurium | 0.25 | 0.1 |
| Pancuronium | 0.06–0.1 | 0.05 |
| Vecuronium | 0.1–0.2 | 0.05 |
Monitoring
▪ Neuromuscular paralysis monitored with peripheral nerve stimulator
□ Objectively monitors degree of skeletal muscle paralysis by determining percentage of neuromuscular receptors “blocked” by the paralytic agent
□ Train-of-four (TOF): stimulus for TOF is delivered as a total of four pulses (low frequency, 2 to 4 Hz, for 2 seconds at 0.5-second intervals); aim is to keep only one or two twitches (of a possible four) visible
□ Tetany: continuous stimulation at either 50 or 100 Hz; sensitive to both residual and deep paralysis; the presence of any persisting strength during tetany is good indicator of the patient’s ability to maintain muscle tone
CESAREAN SECTION IN DOGS AND CATS
Preanesthesia
▪ Preoperative tests depend in part on the age and general health of the pet; in younger otherwise healthy females, minimal tests are needed
▪ In older or unhealthy animals it may be necessary to perform a routine blood count, serum biochemical tests, a urinalysis, and possibly a chest x-ray examination or ECG before anesthesia; the need for such tests varies on a case-by-case basis and depends on the overall health of the pet at the time of anesthesia
▪ Anticholinergics (glycopyrrolate or atropine) decrease salivation and prevent excess vagal tone during uterine traction
▪ Fetal cardiac output is dependent on fetal HR (not blood pressure), and it is imperative to prevent bradycardia by administering an anticholinergic
▪ Atropine crosses the placental barrier and increases fetal HR; glycopyrrolate does not; atropine is the agent of choice in patients undergoing cesarean section
Premedication
| Species | Agents (mg/kg IM; Use Half if Administering IV) |
|---|---|
| Dogs | Oxymorphone 0.05–0.1 ± midazolam (or diazepam) 0.1–0.3 + glycopyrrolate 0.01 |
| Cats | Oxymorphone 0.02–0.08 ± midazolam (or diazepam) 0.1–0.3 + glycopyrrolate 0.01 |
Induction
▪ Propofol is the agent of choice because of rapid clearance, minimal hepatic metabolism, and minimal cardiac depression
▪ Respiratory depression or apnea may occur with large boluses of propofol given rapidly IV; it is recommended that half the calculated induction dose be given over 60 seconds; preoxygenation (oxygen administered via face mask for 5 minutes) before induction prevents maternal and fetal hypoxemia
▪ Monitor ventilation after induction and once patient is placed in dorsal recumbency, as increased abdominal volume may inhibit diaphragmatic movement
Induction
| Species | Agents (mg/kg IV) |
|---|---|
| Dogs | Propofol 4–6 |
| Ketamine 5 + diazepam 0.25 | |
| Thiopental 10 | |
| Mask with isoflurane or sevoflurane | |
| Cats | Propofol 4–6 |
| Ketamine 5 + diazepam 0.25 | |
| Thiopental 10 | |
| Mask with isoflurane or sevoflurane |
Maintenance
▪ Before surgery an epidural block can be performed, but care should be taken not to prolong anesthetic time, as the risk of increased anesthetic time outweighs the benefit of epidural analgesia
Monitoring
▪ Blood pressure should be monitored, and MAP maintained above 60 mm Hg
FELINE DIABETIC PATIENTS
Preanesthesia
▪ Use of sterile technique for catheter placement and surgery is imperative, as diabetic patients are prone to infection
Induction
▪ Propofol has no effect on blood glucose concentration or glucose metabolism; give half the calculated induction dose over 60 seconds; preoxygenate (with oxygen administered via face mask for 5 minutes) before induction to prevent hypoxemia
▪ Ketamine and benzodiazepine induction may lead to tachycardia or arrhythmias and should be used with caution; contraindicated in cats that also have hyperthyroidism



