Chapter 8 Suture plays an important role in wound repair by providing hemostasis and support for healing tissue. Tissues have different requirements for suture support, depending on the type of tissue and anticipated duration of healing. Some tissues need support for only a few days (e.g., muscle, subcutaneous tissue, skin), whereas others require weeks (fascia) or months (tendon) to heal. Individual patient variation further affects suture choice. Healing of wounds may be delayed by infection, obesity, malnutrition, neoplasia, drugs (e.g., steroids), and collagen disorders. In rapidly healing tissue, an ideal suture is one that will lose its tensile strength at a rate similar to that with which the tissue gains strength, and it will be absorbed by the tissue so that no foreign material remains in the wound. Minimally invasive surgical techniques (see Chapter 13) put additional demands on the performance of surgical sutures. Not only must good knot security be maintained, but also the surface lubricant must ensure ease of manipulation, minimal tissue drag, and good biocompatibility with minimal inflammatory responses. Subjective preferences, such as familiarity with the material and availability, need also be taken into consideration when choosing a suture material. The smallest diameter suture that will adequately secure wounded tissue should be used in order to minimize trauma as the suture is passed through the tissue and to reduce the amount of foreign material left in the wound. There is no advantage to using a suture that is stronger than the tissue to be sutured. The most commonly used standard for suture size is the United States Pharmacopeia (USP), which denotes dimensions from fine to coarse (with diameters in inches) according to a numeric scale, with 12-0 being the smallest and 7 the largest. The USP uses different standards for surgical gut and for other materials (Table 8-1). The smaller the suture size, the less tensile strength it has. Stainless steel wire is sized according to the metric or USP scale or by the Brown and Sharpe (B and S) wire gauge (see Table 8-1). The surface characteristics of a suture influence the ease with which it is pulled through tissue (i.e., the amount of friction or “drag”) and the amount of trauma caused. Rough sutures cause more injury than smooth sutures. Smooth surfaces are particularly important in delicate tissues, such as the eye. However, sutures with smooth surfaces also require greater tension to ensure good apposition of tissues and have less knot security (see p. 65). Braided materials have more drag than monofilament sutures. Braided materials often are coated to reduce capillarity (see later discussion), but this also provides a smooth surface. Teflon, silicone, wax, paraffin wax, and calcium stearate are used for coating sutures. Knot tensile strength is measured by the force in pounds that the suture strand can withstand before it breaks when knotted (Box 8-1). Sutures should be as strong as the normal tissue through which they are being placed; however, the tensile strength of the suture should not greatly exceed the tensile strength of the tissue. Terminology Used to Describe Suture Characteristics • Absorbability. Progressive loss of mass and/or volume of suture material; does not correlate with initial tensile strength. • Breaking strength. Limit of tensile strength at which suture failure occurs. • Capillarity. Extent to which absorbed fluid is transferred along the suture. • Elasticity. Measure of the ability of the material to regain its original form and length after deformation. • Fluid absorption. Ability to take up fluid after immersion. • Knot-pull tensile strength. Breaking strength of knotted suture material (10% to 40% weaker after deformation by knot placement). • Knot strength. Amount of force necessary to cause a knot to slip (related to the coefficient of static friction and plasticity of a given material). • Memory. Inherent capability of suture to return to or maintain its original gross shape (related to elasticity, plasticity, and diameter). • Plasticity. Measure of the ability to deform without breaking and to maintain a new form after relief of the deforming force. • Pliability. Ease of handling of suture material; ability to adjust knot tension and to secure knots (related to suture material, filament type, and diameter). • Straight-pull tensile strength. Linear breaking strength of suture material. • Suture pullout value. The application of force to a loop of suture located where tissue failure occurs, which measures the strength of a particular tissue; variable depending on anatomic site and histologic composition (fat, 0.2 kg; muscle, 1.27 kg; skin, 1.82 kg; fascia, 3.77 kg). • Tensile strength. Measure of the ability of a material or tissue to resist deformation and breakage. • Wound breaking strength. Limit of tensile strength of a healing wound at which separation of the wound edges occurs. From Lai SY, Becker DG: Sutures and needles, e-medicine, Topic 38, 2004. Relative knot security is the holding capacity of a suture expressed as a percentage of its tensile strength. The knot-holding capacity of a suture material is the strength required to untie or break a defined knot by loading the part of the suture that forms the loop, whereas the suture material’s tensile strength is the strength required to break an untied fiber with a force applied in the direction of its length (see Box 8-1). Suture materials may be classified according to their behavior in tissue (absorbable or nonabsorbable), their structure (monofilament or multifilament), or their origin (synthetic, organic, or metallic) (Fig. 8-1 and Table 8-2). Two major mechanisms of absorption result in the degradation of absorbable sutures. Sutures of organic origin, such as surgical gut, are gradually digested by tissue enzymes and phagocytized, whereas sutures manufactured from synthetic polymers are principally broken down by hydrolysis. Nonabsorbable sutures are ultimately encapsulated or walled off by fibrous tissue. Characteristics of Suture Materials Commonly Used in Veterinary Medicine *Values given are approximate. Actual loss of tensile strength may vary depending on suture and tissue. †(−), Poor (<60%); (+), fair (60% to 70%); (+ +), good (70% to 85%); (+ + +), excellent (>85%). ‡(−), Minimal to none; (+), mild; (+ +), moderate; (+ + +), severe. Absorbable suture materials (e.g., surgical gut, polyglycolic acid [Dexon, Covidien, Mansfield, Mass.], polyglactin 910 [Vicryl, Ethicon, Somerville, N.J.], polydioxanone [PDS II, Ethicon, Somerville, N.J.], polyglyconate [Maxon, Covidien, Mansfield Mass.], poliglecaprone 25 [Monocryl, Ethicon, Somerville, N.J.], glycomer 631 [Biosyn, Covidien, Mansfield, Mass.]) lose most of their tensile strength within 60 days and eventually disappear from the tissue implantation site because they have been phagocytized or hydrolyzed (see Figure 8-1 and Table 8-2). The time to loss of strength and for complete absorption varies among suture materials. Synthetic absorbable materials (see Table 8-2) generally are broken down by hydrolysis and cause minimal tissue reaction. The time to loss of strength and to absorption is fairly constant even in different tissue. Infection or exposure to digestive enzymes does not significantly influence the rate of absorption of most synthetic absorbable sutures. Polyglactin 910 and polyglycolic acid are more rapidly hydrolyzed in alkaline environments, but they are relatively stable in contaminated wounds. Polyglycolic acid, polyglactin 910, and poliglecaprone 25 may be rapidly degraded in infected urine; polydioxanone, polyglyconate, and glycomer 631 are acceptable for use in sterile bladders and those infected with E. coli. However, any suture that is degraded via hydrolysis may be at risk for accelerated degradation when the bladder is infected with Proteus spp. (see also p. 755), as all common monofilament absorbable sutures have been shown to degrade within 7 days in P. mirabilis–inoculated urine. Polyglycolic acid is braided from filaments extracted from glycolic acid and is available in both coated and uncoated forms. Polyglactin 910 is a multifilament suture made of a copolymer of lactide and glycolide with polyglactin 370. It is coated with calcium stearate and its rate of loss of tensile strength is similar to that of polyglycolic acid. Polysorb (Covidien, Mansfield, Mass.) is a new synthetic absorbable suture material composed of a glycolide/lactide co-polymer. Polysorb has good initial tensile strength and is completely absorbed by 60 days (see Table 8-2). Vicryl Rapide (Ethicon, Somerville, N.J.) is a relatively new, rapidly absorbed, synthetic braided suture that has an initial strength that is comparable to nylon and gut. However, the tensile strength declines to 50% in 5 to 6 days, and it is completely absorbed in 42 days. This suture is indicated for superficial closure of mucosa, gingival closure, and periocular skin closure. Vicryl Plus (Ethicon, Somerville, N.J.) is a new suture that was designed to reduce bacterial colonization on the suture. It has been coated with an antibacterial agent, triclosan. Synthetic nonabsorbable suture materials (see Table 8-2) are marketed as braided multifilament threads (e.g., polyester or coated caprolactam) or monofilament threads (e.g., polypropylene, polyamide, or polybutester). These sutures are typically strong and induce minimal tissue reaction. Nonabsorbable suture materials with an inner core and an outer sheath (e.g., Supramid [S. Jackson, Alexandria, Va.) should not be buried in tissue because they may predispose to infection and fistulation. The outer sheath frequently is broken, which allows bacteria to reside underneath it. The three basic components of a needle are the attachment end (i.e., swaged or eyed end), the body, and the point (Fig. 8-2, A). Eyed needles must be threaded, and because a double strand of suture is pulled through the tissue, a larger hole is created than when swaged suture material is used. Eyed needles may be closed (i.e., round, oblong, or square) or French (i.e., with a slit from the inside of the eye to the end of the needle for ease of threading) (Fig. 8-2, B). Eyed needles are threaded from the inside curvature. The use of eyed needles in veterinary practice has decreased substantially in recent years. With swaged sutures, the needle and suture form a continuous unit, which minimizes tissue trauma and increases ease of use. The needle body comes in a variety of shapes (Fig. 8-2, C); the tissue type and depth and the size of the wound determine the appropriate needle shape. Straight (Keith) needles generally are used in accessible places where the needle can be manipulated directly with the fingers (e.g., placement of purse-string sutures in the anus). Curved needles are manipulated with needle holders. The depth and diameter of a wound are important when selecting the most appropriate curved needle. One-fourth ( The needle point (i.e., cutting, taper, reverse cutting, or side cutting) (Fig. 8-2, D) affects the sharpness of a needle and the type of tissue in which the needle can be used. Cutting needles generally have two or three opposing cutting edges and are designed for use in tissues that are difficult to penetrate, such as skin. With conventional cutting needles, the third cutting edge is on the inside (i.e., concave) curvature of the needle. The location of the inside cutting edge may promote more “cut out” of tissue because it cuts toward the edges of the wound or incision. Reverse cutting needles have a third cutting edge on the outer (i.e., convex) curvature of the needle; this makes them stronger than similarly sized conventional cutting needles and reduces the amount of tissue cut out. Side cutting needles (i.e., spatula needles) are flat on the top and bottom and are generally used for ophthalmic procedures. Taper needles (i.e., round needles) have a sharp tip that pierces and spreads tissues without cutting them. They generally are used in easily penetrated tissues, such as the intestine, subcutaneous tissue, or fascia. Taper-cut needles, which are a combination of a reverse cutting edge tip and a taperpoint body, generally are used for suturing dense, tough fibrous tissue, such as a tendon, and for some cardiovascular procedures, such as vascular grafts. Bluntpoint needles have a rounded, blunt point that can dissect through friable tissue without cutting. They occasionally are used for suturing soft, parenchymal organs, such as the liver or kidney. Muscle has poor holding power and is difficult to suture. Absorbable or nonabsorbable suture material may be used. Sutures placed parallel to the muscle fibers are likely to pull out, so consideration should be given to the type of suture pattern chosen (see p. 75). Suture material used for tendon repair should be strong, nonabsorbable, and minimally reactive. Suturing with a taper or taper-cut needle generally is less traumatic to these tissues. The largest suture that will pass without trauma through the tendon should be used.
Biomaterials, Suturing, and Hemostasis
Sutures and Suture Selection
Suture Characteristics
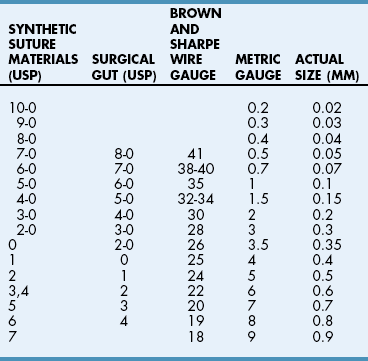
Suture size
Surface characteristics and coating
Knot tensile strength
 Box 8-1
Box 8-1
Relative knot security
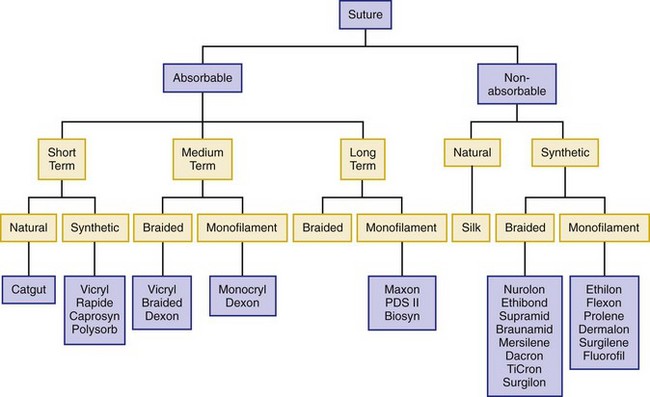
Specific Suturing Materials
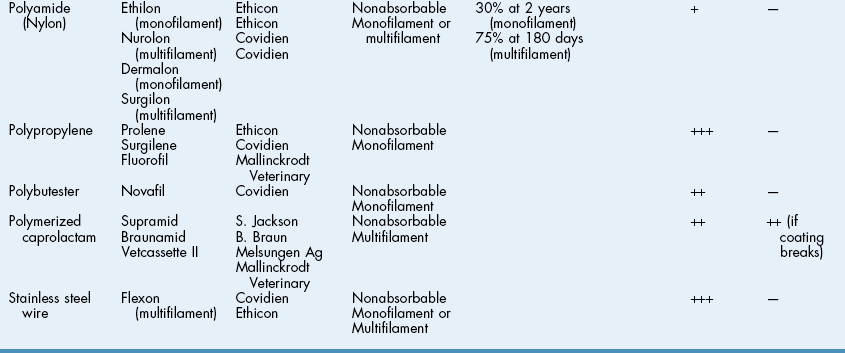
 TABLE 8-2
TABLE 8-2
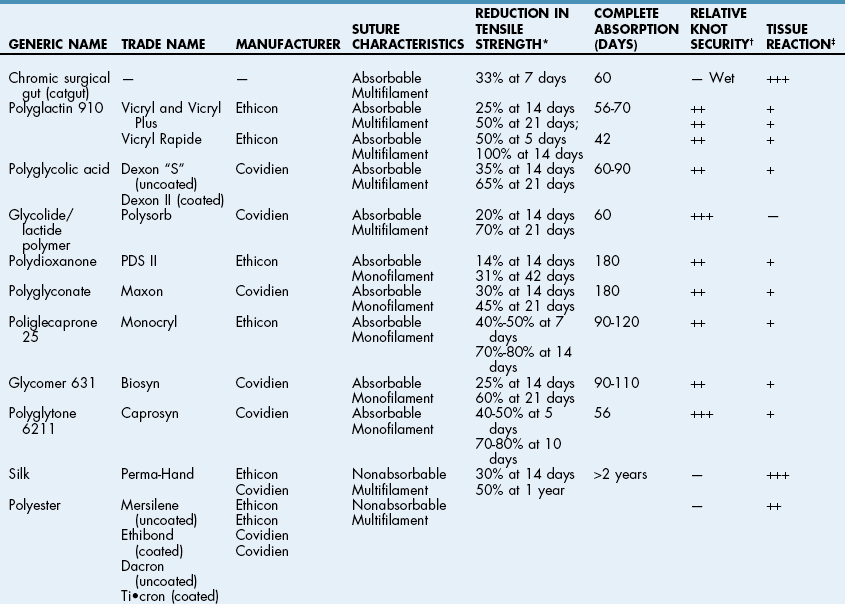
Absorbable Suture Materials
Synthetic absorbable materials
Multifilament absorbable materials
Nonabsorbable Suture Materials
Synthetic nonabsorbable materials
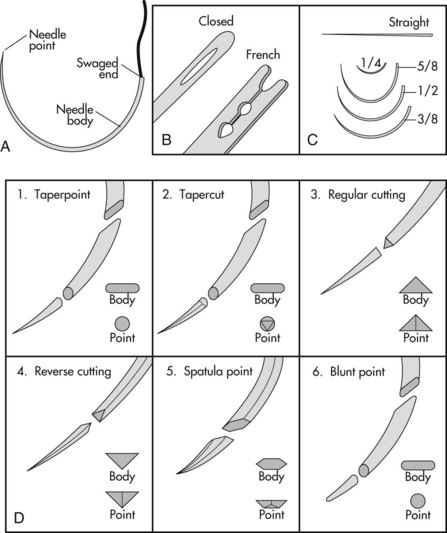
Surgical Needles
 ) circle needles are primarily used in ophthalmic procedures. Three-eighths (
) circle needles are primarily used in ophthalmic procedures. Three-eighths ( ) and one-half (
) and one-half ( ) circle needles are the most commonly used surgical needles in veterinary medicine. Three-eighths circle needles are more easily manipulated than one-half circle needles because they require less pronation and supination of the wrist. However, because of the larger arc of manipulation required, they are awkward to use in deep or inaccessible locations. A one-half circle or five-eighths (
) circle needles are the most commonly used surgical needles in veterinary medicine. Three-eighths circle needles are more easily manipulated than one-half circle needles because they require less pronation and supination of the wrist. However, because of the larger arc of manipulation required, they are awkward to use in deep or inaccessible locations. A one-half circle or five-eighths ( ) circle needle, despite requiring more pronation and supination of the wrist, is easier to use in confined locations.
) circle needle, despite requiring more pronation and supination of the wrist, is easier to use in confined locations.
Suture Selection for Different Tissue Types
Muscle and tendon
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Biomaterials, Suturing, and Hemostasis
 TABLE 8-1
TABLE 8-1