Chapter 171 Avian Respiratory System Disorders
Disorders of the respiratory system are very common in birds. The unique anatomy and physiology of the avian respiratory system can make the diagnosis and treatment of disorders of the respiratory system difficult for the veterinary clinician. This chapter will focus mainly on anatomy, physiology, and clinical management of disorders of the respiratory system of pet parrots. For ease of use, the respiratory system will be discussed based on anatomy, with separation of the upper respiratory tract and lower respiratory tract. Clinical signs of many different disorders are very similar depending on the anatomic location of the disease process.
ANATOMY AND PHYSIOLOGY
Upper Respiratory Tract
• The upper respiratory tract begins at the nares, which are usually located on a fleshy mound at the base of the rhinotheca (upper beak keratin) called the cere.
• The nares open on the dorsal aspect of the cere into the nasal cavity. An operculum is present just within the nasal opening in Amazon parrots (Amazona species) that probably functions in filtering out particulate matter.
• The nasal cavity is divided by a septum and is composed of three fairly distinct and well-vascularized conchae—rostral, middle, and caudal. The middle concha is the largest of the three in most parrots.
• The nasal cavity opens into the dorsal aspect of the oral cavity via the choanal slit. The choanal slit is normally lined by a respiratory epithelium and, grossly, sharp papillae can be seen extending into the lumen of the slit from the lateral margins. Absence of these choanal papillae is a sign of respiratory pathology.
• During breathing, the larynx abuts the choanal slit to allow close-mouthed nasal breathing in a normal parrot.
• The infraorbital sinus is the only sinus in birds, but it is quite large and convoluted, with six diverticula that can be found anatomically throughout the head and beak.
• The dorsal aspect of the infraorbital diverticulum opens into the middle and caudal nasal conchae. This dorsal opening makes drainage of the sinus difficult in a clinical setting.
• The rima glottidis is not covered by an epiglottis, as is the case in mammals. Paired arytenoids cartilages form the walls of the rima glottidis.
• Compared with that of mammals, the avian trachea and rima glottidis are quite wide in diameter relative to the size of the bird. In addition, the trachea is long and often convoluted as it tracks down the neck. This convolution allows the bird full range of flexibility in the neck.
• Because of the large diameter and length of the trachea, there is a larger physiologic dead space in birds compared with in mammals. To compensate for this, birds tend to have a slower respiratory rate but a larger tidal volume.
• At the bifurcation of the trachea (at the thoracic inlet in most parrots), the syrinx can be found. The syrinx is the sound-production organ of the bird, and it is an important anatomic structure as it is a common location of many disease processes, including inhaled foreign bodies and fungal granulomas. The syrinx is composed of a number of complex cartilages, muscles, and membranes that work together to create vibrations that can be amplified to create loud sounds.
Lower Respiratory Tract
• The lungs are paired, non-expansible, and located against the dorsal body wall in the thoracic region of the coelom.
• The parabronchi travel throughout each lung and have extensive anastomoses with each other. The parabronchi have outpocketings throughout their length, termed atria, which further open into infundibula. The infundibula narrow in size into air capillaries, the functional equivalent of the mammalian alveoli. Gas exchange occurs throughout the anastomosing meshwork of the air capillaries, which course in immediate proximity to the blood capillaries.
• To complete a respiratory cycle, birds require two breaths. On the first inhalation, the majority of inhaled air moves into the caudal air sacs. On the first exhalation, this air then moves through the lungs, where gas exchange occurs. On the second inhalation, the air in the lungs moves to the cranial air sacs, and on the second expiration, this air is then expelled through the trachea. This unidirectional flow of air makes up the majority of respiration in pet parrots.
• Bidirectional flow also occurs in parrots, wherein a small percentage of inhaled air goes directly to the lungs and is then expelled on expiration. Because of these two systems, birds exchange gas on both inspiration and expiration.
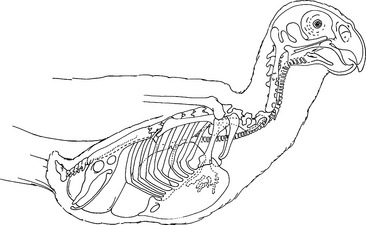
• Birds lack a diaphragm; they rely on a system of bellows, the air sacs, to propel air throughout the respiratory tract. Pressure changes in the air sacs are a result of muscle-controlled volume changes within the thoracoabdominal coelom (see Fig. 171-1).
• Parrots have nine air sacs: paired cervicocephalic, single clavicular, paired cranial thoracic, paired caudal thoracic, and paired abdominal. The latter four sets of air sacs have connections to the lungs (termed ostia), so they are considered part of the lower respiratory tract. As discussed above, the cervicocephalic air sacs have connections to the infraorbital sinus but not the lungs.
• Histologically, air sacs are similar to peritoneum: one to two cell layers thick, relatively avascular, and composed of connective tissue stroma.
• In some species, the air sacs extend into the bones. In parrots, the only consistently pneumatic bone is the humerus, which is aerated by the clavicular air sac.
CLINICAL SIGNS OF RESPIRATORY DISORDERS
Upper Respiratory Tract
• Common historical and physical examination findings in parrots with nasal, sinus, or choanal disorders include the following:
DISORDERS OF THE UPPER RESPIRATORY TRACT
Hypovitaminosis A
Clinical Signs
• Most commonly, parrots present with chronic sinusitis due to secondary infections and blunted choanal papillae.
Treatment
• Correct the diet by recommending a formulated pelleted diet, fresh food diet, or some combination of the two. Seeds should be fed in a minute quantity if at all.
• Treat secondary infections with appropriate antimicrobials; trimethoprim-sulfa (25 mg/kg PO q12h) or enrofloxacin (20 mg/kg PO q24h) are good first-line choices until culture results are obtained.
• Give a single injection of vitamin A (10,000 IU/kg IM). Vitamin A is often available combined with vitamins D and E. Dosing should be made on the vitamin A component of this mixture. No more than two injections given 1 week apart should be recommended, as oversupplementation of vitamin A can have serious deleterious effects.
• Supplement the diet with beta carotene (one to two drops per parrot) while the bird is being converted to a healthier diet. Beta carotene is a precursor to formed vitamin A and overdosage is unlikely, as parrots will excrete what they do not need. Owners can monitor for orange or yellow discoloration of the urine, which occurs when beta carotene is being supplemented in excess. Supplementation with formed vitamin A is not recommended due to the likelihood of overdosage. Signs of hypervitaminosis A are similar to those of hypovitaminosis A.
Rhinitis
Diagnosis
• Obtain a thorough dietary and environmental history, paying particular attention to airborne irritants.
Treatment
• See the section on hypovitaminosis A for good first-choice antimicrobials or a base choice on cytologic findings.
• If the diet is deficient in vitamin A, correction of the diet should be part of the therapeutic plan.
• Control environmental irritants by use of air filtration, humidification, and adequate ventilation.



