Chapter 39 Avian Circovirus and Polyomavirus Diseases
Psittacine Beak and Feather Disease
PBFD, arguably the most recognizable disease of Psittaciformes, is a major problem of wild psittacine birds in Australasia and in captive birds worldwide. The disease was first recorded in wild Australian sulfur-crested cockatoos (Cacatua galerita) in 1903,16,17 and a second report in 19072 described feather disease affecting red-rumped parrots (Psephotus haematonotus) in South Australia. Affected birds were described as “quite healthy, except being destitute of feathers.” PBFD has since come to be recognized as the most common disease of wild and captive psittacine birds, with a worldwide distribution, and posing a threat to the conservation of endangered psittacine birds in Australia, South Africa, and New Zealand.
Clinical Signs
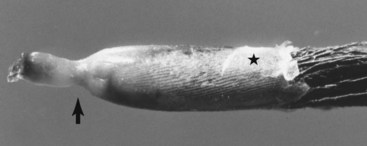
More commonly, PBFD develops as a chronic disease that is insidious in its development and progression; dystrophic feathers replace normal ones as they are molted. In this manner, a PBFD-affected bird may gradually lose its plumage without other signs of illness (Fig. 39-1). The pattern of feather dystrophy is related to the stage of molt that the bird is in when the disease first begins; it is usually bilaterally symmetrical and slowly progressive. Dystrophic feathers are usually short and have one or more of the following characteristics: fault lines across the vanes; a thickened or retained feather sheath; blood within the calamus; an annular constriction of the calamus; and curling (Fig. 39-2).

Diagnosis
Virus detection by hemagglutination (HA) assay is a sensitive diagnostic test for detecting BFDV antigen emission in feather material. Chronically affected birds typically excrete very high titers (>1 : 40,960), often in the absence of detectable antibodies measurable by hemagglutination inhibition (HI) assay.10 HA may be used to detect virus excretion in feathers, liver, bile, and feces and may be performed on actively growing feather pulp or dry keratinized feathers.
Virus DNA detection by polymerase chain reaction (PCR) assay is also available as a diagnostic test and may detect BFDV infection in circulating leucocytes or feather material. The results must be interpreted in relation to the clinical signs and results of other tests, because cross-contamination caused by unclean collection and laboratory technique is possible.4,10,12
Serology may be done by HI, enzyme-linked immunosorbent assay (ELISA), or blocking ELISA (bELISA) and is useful for detecting BFDV-infected flocks or seroconversion in individual birds.8,10,24 A high plasma HI antibody titer (>1:320) in an adult bird is a good indicator that it does not have chronic PBFD. Nestlings with incubating infection or acute disease may have low and declining antibody titers. The HI test may be done on serum, plasma, or whole blood collected on filter paper.
Pathogenesis and Epidemiology
Very little is known about the steps involved in the replication of BFDV but it is possible that it uses a similar mechanism for cellular entry into macrophages as that discovered for porcine circovirus The capsid protein contains a nuclear localization signal that assists viral entry into the nucleus,7 but the genome may also be able to enter the nucleus during mitosis by associating itself with cellular chromatin. Circoviruses are highly dependent on cellular enzymes for their replication via the synthesis of a complementary strand to form a double-stranded DNA (dsDNA) replicative form and then by rolling circle replication. How assembled virions are transported into the nucleus to form the characteristic paracrystalline arrays, which are readily seen histologically, is not precisely known, but BFDV Cap and Rep are known to interact,7 which may facilitate transport of encapsidated virions into the cytoplasm.
The maximum incubation period of PBFD is unknown, because the appearance of clinical signs depends on the stage of molt of the bird; however, experimentally infected nestlings may show signs of acute disease from 21 to 28 days postinfection. BFDV is excreted via the feathers and the gastrointestinal tract. Consequently, high concentrations of BFDV antigen may be detected in liver tissue, bile, crop secretions, feces, and feather dander. Horizontal transmission by oral and/or intracloacal ingestion of virus excreted via feces, feather dander, and crop secretions is likely the primary mechanism of viral spread. Experimental infection may also be accomplished by intramuscular administration of the virus. Vertical transmission is suspected, because BFDV DNA has been amplified from embryonated eggs by PCR assay.18
All species of psittacine birds should be considered to be susceptible to BFDV. Depending on the species and age, not all birds infected with BFDV progress to develop clinical signs of disease. Spontaneous clinical recovery from acute PBFD may occur rarely in many species, including budgerigars (Melopsittacus undulatus), lorikeets, and Eclectus and Agapornis spp. but these birds typically become carriers. However, most chronically affected birds do not recover from the disease. Individual lorikeets and eclectus parrots may develop protective HA antibody with intermittent cessation of virus excretion. In contrast, others, such as African grey parrots and black cockatoos (Calyptorhynchus and Callocephalon spp.), appear highly susceptible and may die before clinical signs of feather loss develop. In contrast, cockatiels seem to be resistant to BFDV infection and subsequent PBFD.23 White cockatoos (Cacatua spp.) typically develop the chronic form of the disease, with high HA titers detectable in feathers and feces and no detectable HI titer. The reasons for the variations in clinical disease remain to be explained.
Compared with APV, BFDV is a relatively genetically diverse species, with BFDV nucleotide sequence similarities reported to range from 84% to 99%. Based on phylogenetic analyses and differences in pathogenicity, the existence of strains of BFDV has been proposed but this has yet to be confirmed experimentally. Individual serotypes were not found in the one cross-reactivity study10 undertaken to date. However, studies on BFDV isolates from PBFD-affected cockatiels (Nymphicus hollandicus) have shown some degree of serologic and phylogenetic divergence, but this is insufficient to justify classifying these as distinct strains or species.23
In infected flocks viral DNA may be detected in up to 28.0% of birds6 in wild flocks and up to 83% to 90% of birds in captive flocks.10 Seroprevalences up to 62% in captive flocks and up to 94% in wild flocks have been reported. In wild birds, PBFD has been confirmed in most Australian psittacine bird species, as well as in parrots and cockatoos throughout Indonesia, Papua New Guinea, and New Zealand. In Australia, flocks of wild cockatoos may have a disease prevalence of 20% and a seroprevalence of 60% to 80% and infection is probably maintained in a population by diseased birds and contaminated nest hollows. Epidemics may occur in susceptible wild or aviary flocks. Virus transmission is probably predominantly by horizontal spread, but carrier birds may contribute by vertical transmission. Virus infectivity probably persists in contaminated nests for many months or years. Aviary flocks with a history of PBFD usually have a high seroprevalence. In these situations, PBFD-affected birds are often the progeny of hens with low or nondetectable serum antibody levels.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


