3.1 Scapula52
3.2 Shoulder53
3.3 Humerus55
3.4 Elbow55
3.5 Radius and ulna (antebrachium, forearm)60
3.6 Carpus63
3.7 Metacarpus, metatarsus and phalanges65
3.8 Pelvis and sacroiliac joint67
3.9 Hip (coxofemoral joint)68
3.10 Femur71
3.11 Stifle71
3.12 Tibia and fibula77
3.13 Tarsus (hock)77
This chapter describes conditions that are most commonly associated with specific bones or joints. Lack of inclusion of a condition under an anatomical area may not mean that it cannot occur there, simply that this area is not a predilection site; for example synovial sarcomas most often arise around the elbow and stifle, although they may arise near any synovial joint. Conditions that may occur in any joint (e.g. infectious arthritis) are described in Chapter 2, Joints.
For each anatomical area, the conditions are listed in the following order:
• artefacts and normal anatomical variants
• congenital or developmental
• metabolic
• infective
• inflammatory
• neoplastic
• traumatic
• degenerative
• miscellaneous conditions.
Conditions that most closely resemble each other radiographically are indicated by ‘differential diagnosis’. Conditions involving joints are listed under the relevant bone but described more fully under the appropriate joint.
Joint trauma tends to affect the weakest area, hence physeal fractures occur in skeletally immature animals and ligamentous damage in older animals; young dogs rarely suffer from ligament trauma.
In many cases in which there is doubt as to the presence of genuine pathology, always consider radiographing the opposite limb for comparison.
Useful terminology
Brachymyelia – abnormally short limb.
Dimelia – duplication of a limb.
Dysmelia – congenital deformity of a limb.
Ectromelia – absence of part of a limb.
Hemimelia – absence of the distal part of a limb; also used to denote absence of radius or ulna or tibia or fibula.
Meromelia – incomplete limb development.
Micromelia – abnormally small limb.
Notomelia – accessory limb attached to the back.
Peromelia – as dysmelia.
Phocomelia – absence of the proximal portion of a limb.
Adactyly – absence of a digit.
Brachydactyly – reduced size of outer digits.
Dactomegaly – abnormally large digit.
Ectrodactyly – absence of part or all of a digit; also used to describe split hand (lobster claw) deformity.
Polydactyly – supernumerary digit(s).
Polymyelia – supernumerary limb.
Polypodia – supernumerary feet.
Syndactyly – fusion of digits.
Valgus – lateral deviation of a limb distal to an abnormal growth plate or fracture malunion.
Varus – medial deviation of a limb distal to an abnormal growth plate or fracture malunion.
Ultrasonography of the musculoskeletal system
The use of ultrasonography is now well documented for investigation of musculotendinous lesions, although it requires considerable experience. High-frequency transducers of 7.5 MHz or more are required, and linear transducers give contact over a larger area.
The appearance of a normal tendon in longitudinal section is a band of medium echogenicity with parallel hyperechoic lines representing the fibrillar texture of the tendon, and in transverse section is of a round to ovoid structure with central inhomogeneities. The peritenon appears as a hyperechoic, continuous line. Acute and chronic tendinitis, tenosynovitis, mineralization, partial or complete tendon ruptures and tendon dislocations can be detected, and tendon healing after injury can be monitored.
Normal muscle is hypoechoic to anechoic with fine, oblique echogenic striations. Muscle injuries can be detected, their appearance varying with age of the injury; as with tendons, healing can be monitored.
Joints may be assessed ultrasonographically provided that an acoustic window can be found, although often only small areas can be seen. The bone surface, articular cartilage, synovium and synovial fluid may be recognized, but ligaments are usually too small to see. Joint effusion, chronic synovitis, articular cartilage defects, joint mice, chronic synovitis and osteophytes may be identified.
Ultrasonography may be used to examine the surface of bones and soft tissue lesions such as abscesses, haematomas, foreign bodies and soft tissue tumours, allowing ultrasound-guided aspiration in many cases.
See the further reading list for more information.
3.1. SCAPULA
Views
Mediolateral (ML); ML with dorsal displacement of the limb; caudocranial (CdCr); distoproximal – dorsal recumbency with the affected limb pulled caudally so the scapula is vertical and the shoulder joint is flexed to 90°.
Development
The ossification centre of the scapular body is present at birth, and the scapular tuberosity appears at 7 weeks; fusion occurs at 4–7 months.
1. Ossification centre of the scapular tuberosity (supraglenoid tubercle) fuses to the body of the scapula by 4–7 months; differential diagnosis is fracture.
2. Chondrosarcoma – flat bones are predisposed (scapula, pelvis, cranium, ribs).
3. Scapular fractures. Usually young, medium to large breeds of dog and after major trauma; often concurrent thoracic injuries.
a. Scapular body – non-articular.
b. Scapular spine – non-articular.
c. Scapular neck – non-articular.
d. Scapular tuberosity (supraglenoid tubercle) – usually avulsed by biceps brachii tendon in skeletally immature animals, articular; differential diagnosis is separate centre of ossification.
e. Other glenoid fractures; articular.
3.2. SHOULDER
Views
ML; ML with pronation and/or supination; CdCr; flexed cranioproximal–craniodistal oblique (CrPr–CrDiO) for the intertubercular groove through which biceps tendon runs; arthrography (see 2.1). On the CdCr view, the joint space is often wider medially.
Ultrasonography
The use of ultrasonography for shoulder disease has been described (see Further reading).
1. Clavicles – clearly seen in cats; smaller and less mineralized in dogs, but rudimentary structures are sometimes visible, especially on the CdCr view of the shoulder; bilaterally symmetrical.
2. Caudal circumflex humeral artery seen end on caudoventral to the joint, surrounded by fat; differential diagnosis is poorly mineralized joint mouse.
3. Separate ossification centre of glenoid – small, crescentic mineralized opacity adjacent to the caudal rim of the glenoid; may fuse to the scapula or persist throughout life; may be an incidental finding but differential diagnosis is osteochondrosis (OC) of glenoid (see 3.2.5 below). However, incomplete ossification of the caudal glenoid has recently been reported as causing lameness in a number of larger breed dogs of varying ages, especially the Rottweiler. Possibly associated with minor trauma, abnormal growth and OC (or osteochondritis dissecans, OCD). Damage to the medial glenohumeral ligament may also be present. Radiographs show a bony fragment adjacent to the caudal glenoid margin ± secondary osteoarthrosis.
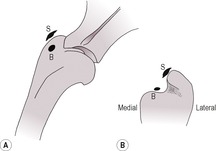
4. Osteochondrosis of the humeral head; also called OCD if there is evidence of cartilage flap formation (Fig. 3.1) – young dogs mainly 5–7 months old of larger breeds; Border Collies, Labradors and Great Danes over-represented; male preponderance; often bilateral. Reported only twice in cats. Radiographic signs include flattening or concavity of the caudal third of the humeral articular surface ± subchondral lucency or sclerosis, overlying mineralized cartilage flap. In chronic cases joint mice may be seen, usually in the caudal joint pouch but also in the biceps tendon sheath or the subscapular joint pouch (CdCr view), as well as mild secondary osteoarthrosis. The presence of the vacuum phenomenon (see 2.2.13) is highly suggestive of an OC lesion. Arthrography is helpful in demonstrating thickening and irregularity of the articular cartilage layer, non-mineralized cartilage flap formation and non-mineralized joint mice. Ultrasonography can also be used to show OCD lesions, joint mice, joint effusions and new bone.

5. Osteochondrosis of the glenoid rim – unusual – separate mineralized fragment adjacent to articular rim; differential diagnosis is separate centre of ossification, but usually larger.
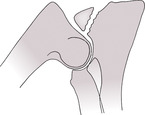
6. Congenital shoulder luxation or subluxation (Fig. 3.2) – rare, mainly miniature and toy breeds of dog, especially the Toy Poodle; may be bilateral. Usually present at 3–10 months of age, but older animals may show luxation after minor trauma. The humerus is normally displaced medially due to underdevelopment of the medial labrum of the scapular glenoid, but spontaneous reduction may occur on positioning for radiography. Radiographic signs include a flattened, underdeveloped glenoid with progressive remodelling of articular surfaces leading to osteoarthrosis; differential diagnosis is trauma at an early age.

7. Traumatic shoulder luxation – uncommon, unilateral. The humerus is usually displaced medially or laterally, occasionally cranially or caudally. With sagittal displacement, ML radiographs show a slight overlap of the scapula and humerus with loss of the joint space; on CdCr radiographs, the luxation is obvious unless spontaneous reduction has occurred; differential diagnosis is normal medial widening of the shoulder joint space on a CdCr view, especially if poorly positioned and particularly in smaller dog breeds. Check also for associated chip fractures.
8. Fractures involving the shoulder joint.
a. Scapular tuberosity (supraglenoid tubercle) – Salter–Harris type I growth plate fracture in a skeletally immature animal, or bone fracture in a mature animal. May be avulsed by biceps brachii tendon. Differential diagnosis is separate centre of ossification.
b. Other articular glenoid fractures.
c. Salter–Harris type I fracture of the proximal humeral epiphysis in young animals – rare.
d. Articular fracture of the proximal humeral epiphysis – rare.
9. Biceps brachii tendon rupture – acute or gradual onset; partial or complete; Bernese Mountain Dog and Rottweiler predisposed. Diagnosed by positive contrast arthrography or ultrasonography. With ultrasonography of complete tendon rupture, there is an area that is hypo- to anechoic due to bleeding between the tendon ends, which are swollen, hyperechoic and heterogeneous. With partial rupture, the tendon is swollen and of irregular echotexture with tendon sheath effusion.
10. Biceps brachii tendon sheath rupture – reported in two Labradors. Rupture of the tendon sheath distally, diagnosed by positive contrast arthrography that showed leakage of contrast medium distally, outlining the proximal part of the muscle belly.
11. Shoulder osteoarthrosis – usually osteophytes on the caudal glenoid rim and caudal articular margin of the humeral head. The amount of new bone formation is often relatively mild. Joint mice may be visible in the caudal joint pouch and may become very large in old dogs. Some may develop into synovial osteochondromas.
a. Primary – ageing change; often clinically insignificant.
b. Secondary – for example following OC (OCD).
12. Calcifying tendinopathy – usually supraspinatus and biceps brachii tendons (Fig. 3.3); changes in the infraspinatus tendon and bursa and coracobrachialis tendon are also reported. Mainly medium to large, middle-aged dogs, especially Rottweilers and Labradors; aetiology unknown. Mild, chronic or intermittent lameness or clinically silent. May be bilateral. Radiographic signs include areas of mineralization in the region of the affected tendon or bursa; differential diagnosis is rudimentary clavicles or joint mice in the biceps tendon sheath. Orthogonal radiographs (ML and CdCr) are essential to differentiate lesions within the bicipital groove from those medial or lateral to the shoulder, and the CrPr–CrDiO view and arthrography are also helpful in identifying the tendon of origin. Radiographs of the opposite shoulder should be obtained for comparison. Bicipital calcifying tendinopathy may be associated with tenosynovitis (see 3.2.13). Ultrasonography of the tendons may be helpful in showing fibre disruption, areas of mineralization (hyperechoic foci with distal acoustic shadowing) and joint capsule or tendon sheath effusion.
13. Bicipital tenosynovitis and bursitis – signalment as above. Radiographs may be normal or may show ill-defined sclerosis and new bone in the intertubercular groove, enthesiophytes on the supraglenoid tubercle and mild osteoarthrosis. Arthrography may show reduced or irregular filling of the biceps tendon sheath due to synovial villous hypertrophy. Ultrasonography may be used to demonstrate fluid distension of the bursa and tendon sheath and changes within the tendon itself.
3.3. HUMERUS
Views
ML; CdCr or craniocaudal (CrCd).
Development
The ossification centre of the humeral diaphysis is present at birth, and the proximal epiphysis appears at 1–2 weeks. Fusion of the greater tubercle to the humeral head occurs at 4 months and of the proximal epiphysis to the diaphysis at 10–13 months. At the distal end of the bone, the ossification centres of the medial and lateral parts of the humeral condyle appear at 2–3 weeks and of the medial epicondyle at 6–8 weeks; the two halves of the condyle fuse at 8–12 weeks, the medial epicondyle at 6 months and the condyle to the diaphysis at 5–8 months.
1. Compensatory overgrowth of the humerus – increase in humeral length compared with the contralateral limb has been described in dogs in which there is significant antebrachial shortening due to premature closure of radial and/or ulnar growth plates. The mechanism is thought to be secondary to either reduced physeal compression as a result of decreased weight bearing, or alteration in blood flow.
5. Humeral fractures.
a. Distal two-thirds of diaphysis – commonest area; usually spiral or oblique and may be comminuted, following the musculospiral groove; commonly associated with transient radial paralysis.
b. Proximal third of diaphysis – usually a transverse fracture near the deltoid tuberosity.
c. Salter–Harris type I fracture of the proximal humeral growth plate in skeletally immature animals.

3.4. ELBOW
Views
Flexed, extended and neutral ML; CrCd; CdCr, although results in magnification and blurring; craniolateral–caudomedial oblique (CrL–CdMO); craniomedial–caudolateral oblique (CrM–CdLO); arthrography. Oblique views may be obtained by pronating or supinating the limb.
Ultrasonography
Normal ultrasonographic anatomy of the canine elbow has been described (see Further reading).
2. Elbow sesamoids – mineralized elbow sesamoids are commonly seen in both dogs (mainly larger breeds) and cats; small, smooth, round bodies craniolateral to the radial head; usually bilateral. Mainly in the supinator muscle but also reported in the annular ligament and lateral collateral ligament. Differential diagnoses are joint mice, chip fractures; should not be confused with a fragmented medial coronoid process.
3. Absence of the supratrochlear foramen of the distal humerus – occasionally noted in small, chondrodystrophic breeds of dog.
4. Cats – the supracondylar foramen is present on the medial aspect of the distal humerus and is visible on a CrCd or CrL–CdMO radiograph; the brachial artery and median nerve pass through this foramen.
5. Incomplete ossification of the humeral condyle (Fig. 3.4) – especially English Springer Spaniels and American Cocker Spaniels but also seen in other Spaniel breeds and crosses and in some other pure breeds; male preponderance; often bilateral. Failure of fusion of the medial and lateral centres of ossification in the condyle results in a residual sagittal cartilaginous plate that may be clinically silent or cause lameness in its own right as well as predisposing to condylar fractures (see 3.4.17 and Fig. 3.10). The fissure may be seen on CrCd or Cr 15° M–CdLO radiographs when the X-ray beam is parallel to the fissure, extending proximally from the articular surface to the physis and sometimes beyond into the supratrochlear foramen. Differential diagnosis is Mach effect along the edge of the superimposed olecranon (see 1.9).
6. Coronoid disease: fragmentation of the medial coronoid process of the ulna (FMCP) (Fig. 3.5) – part of the elbow dysplasia complex seen in young dogs of medium and large breeds, especially the Labrador, Golden Retriever, Bernese Mountain Dog, Rottweiler, Newfoundland; male preponderance; often bilateral. Lameness is first seen from 4–12 months of age. In some cases, initial lameness is not detected, particularly if bilateral disease is present, and the dog presents at an older age with osteoarthrosis. Predisposed to by elbow incongruity with widening of the humeroradial joint space, which puts increased pressure on the medial coronoid process. The diagnosis of FMCP and of humeral condylar OC is often made by identification of secondary osteoarthrosis in an appropriate patient rather than by visualization of a primary lesion (see 3.4.19 and Fig. 3.11); a specific diagnosis may not be possible without arthrotomy, arthroscopy or high-resolution CT or magnetic resonance imaging. The primary radiographic findings are flattening, rounding or fragmentation of the process on the ML and Cr 15° L–CdMO views; the CrCd view shows not the process itself but a more medial projection of bone, which may be remodelled. ‘Kissing’ subchondral lesions may also be seen on the opposing articular surface of the humeral condyle; differential diagnosis is humeral OC (OCD).

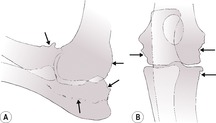
7. Osteochondrosis (OCD) of the medial part of the distal humeral condyle (Fig. 3.6) – also part of the elbow dysplasia complex affecting the same breeds as above but with no gender predilection; often bilateral. The primary lesion is best seen on the CrCd view as subchondral bone flattening or irregularity, subchondral sclerosis, ± overlying mineralized cartilage flap; severe lesions may also be visible on the ML view; differential diagnosis is kissing lesion created by a fragmented medial coronoid process. Osteoarthrosis develops as with FMCP.

8. Ununited anconeal process (Fig. 3.7) – also part of the elbow dysplasia complex, although mainly in the German Shepherd Dog, Irish Wolfhound, Great Dane, Gordon Setter and Basset Hound; no gender predilection; often bilateral. Predisposed to by elbow incongruity with a slightly shorter ulna or longer radius putting pressure on the anconeus, but may also be due to trauma; some cases are bilateral. The separate centre of ossification for the anconeus usually fuses to the ulna between 3 and 5 months, and persistence of a radiolucent cleavage line beyond this time indicates separation. The flexed ML view is diagnostic, showing a substantial triangular bone fragment either adjacent to ulna or displaced proximally; chronic cases showing remodelling of the fragment and/or osteoarthrosis.
9. Elbow incongruity – seen in the various breeds predisposed to elbow dysplasia but especially in the Bernese Mountain Dog. Poor congruity between the humerus, radius and ulna puts increased pressure on the medial coronoid process or the anconeus and may lead to fragmentation or separation of these processes, respectively. Usually the humeroradial joint space is widened, best assessed on a CrCd view, as it is quite position-sensitive. May be seen alone or with FMCP, OC, ununited anconeal process ± osteoarthrosis. The clinical significance of incongruity alone is uncertain.
10. Medial epicondylar spurs (flexor tendon enthesiopathy) (Fig. 3.8) – usually larger breed dogs; may be bilateral; aetiology and significance not known and in some dogs is an incidental radiographic finding. The ML radiograph shows a distally projecting bony spur on the caudal aspect of the medial humeral epicondyle, or less commonly linear mineralization in adjacent soft tissues.

11. ‘Ununited medial epicondyle’ – unusual; aetiology not known but may be part of the elbow dysplasia complex, as similar breeds are affected, mainly young Labradors; may be bilateral. Single or multiple mineralized fragments of varying size and shape are seen at several locations near the medial epicondyle, sometimes with an adjacent bone defect. Secondary osteoarthrosis may be very minor. Some cases are radiographically similar to flexor enthesiopathies, and these may be different manifestations of the same condition.
Box 3.1 describes the grading system recommended by the International Elbow Working Group for elbow dysplasia screening.
BOX 3.1
The International Elbow Working Group recommends the following grading system for elbow dysplasia screening based on the degree of secondary osteoarthrosis, from 12 months of age onwards:
▪ grade 0 – normal elbow, no osteoarthrosis or primary lesion
▪ grade 1 – mild osteoarthrosis with osteophytes < 2 mm
▪ grade 2 – moderate osteoarthrosis with osteophytes 2–5 mm
▪ grade 3 – severe osteoarthrosis with osteophytes > 5 mm.
Primary lesions described include malformed or fragmented medial coronoid process, ununited anconeal process, osteochondrosis (osteochondritis dissecans) of the humeral condyle and incongruity of the articular surfaces. Grading schemes in different countries vary in the number of radiographic views required and in their grading of primary lesions; the minimum requirement is a flexed mediolateral view of each elbow.
12. Elbow subluxation.
a. Severe elbow incongruity (see 3.4.9).
b. Secondary to relative shortening ± curvature of the ulna or radius, usually due to traumatic lesions at the distal growth plates or chondrodysplasia, and therefore recognized in young animals (see 4., 5., 6. and 7.). Shortening of the ulna causes widening of the humeroulnar space distally and increased pressure on the anconeal process; shortening of the radius causes widening of the humeroradial space and of the humeroulnar space proximally, resulting in increased pressure on the medial coronoid process of the ulna.
c. Distractio cubiti or dysostosis enchondralis in chondrodystrophic breeds (see 3.5.5).
d. Congenital humeroulnar (sub)luxation – mainly small breeds of dogs (e.g. Pekinese) but also cats; male preponderance; often bilateral. Deformity is severe, with obvious limb dysfunction, and is therefore recognized at an early age (3–6 weeks). There is lateral displacement and 90° medial rotation of the ulna with a normal humeroradial articulation; the elbow is held in flexion and the distal limb is pronated. Radiographically, the ulna is displaced laterally so its trochlear notch faces medially and is seen in profile on a CrCd view of the elbow; affected areas of bone are remodelled, and in chronic cases, osteoarthrosis develops.
e. Congenital or developmental displacement of the radial head (Fig. 3.9) – mainly larger breeds of dog with no gender predilection; may be bilateral. May also be secondary to growth disturbances of the distal radius and ulna. Deformity is milder than with humeroulnar subluxation, although progressive degenerative joint changes develop. The radial head is (sub)luxated laterally or caudolaterally and is remodelled; the radius may appear longer than normal.

f. Congenital complex elbow (sub)luxation – may be seen with other deformities such as ectrodactyly and split hand deformity (see 3.7.7).
13. Patella cubiti – a rare fusion defect through the trochlear notch of the ulna such that the olecranon and proximal ulnar metaphysis are separated from the rest of the ulna and distracted by the triceps muscle; so-called because the fragment of bone is patella-shaped. May be bilateral. Differential diagnosis is avulsion fracture through the proximal ulnar growth plate or trochlear notch.
15. Synovial sarcoma (occasionally other soft tissue tumours, such as histiocytic sarcoma; see 2.4.7 and Fig. 2.4) – the elbow is a predilection site; mainly larger breeds of dog; differential diagnoses are severe osteoarthrosis, in which superimposition of new bone may mimic osteolysis; septic arthritis. The diagnosis may be difficult in cases in which tumour is superimposed over pre-existing osteoarthrosis. In the case of a tumour, a soft tissue mass may be palpable or radiographically visible adjacent to the joint.
17. Fractures involving the elbow joint.
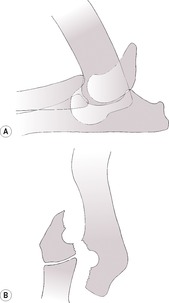
a. Lateral humeral condylar fracture (Fig. 3.10) – usually Spaniels and Spaniel crosses; often minor trauma only; may be bilateral. Young dogs or adults; in the latter, thought to be predisposed to by incomplete ossification between the medial and lateral parts of the humeral condyle (see 3.4.5 and Fig. 3.4), together with the increased loading of the lateral part of the condyle by its articulation with the radius and its weak attachment to the humeral shaft. Best seen on the CrCd view, but overriding of the fragments is also seen on the ML view. The most common elbow fracture, because the lateral condyle articulates with the radius and takes most of the load, and also because its epicondyle is relatively insubstantial.
b. Y fractures of the humeral condyle – also Spaniels and predisposed to by incomplete ossification of the humeral condyle; the fracture line runs proximally between the medial and lateral parts of the condyle into the supracondylar foramen, and then separate fracture lines emerge through the medial and lateral humeral cortices. Best seen on the CrCd view.
d. Salter–Harris type I fracture of the distal humeral epiphysis in skeletally immature animals – uncommon.
e. Olecranon fractures – through the proximal ulnar physis in skeletally immature animals (non-articular) or into the trochlear notch (articular), both with distraction by triceps muscle; differential diagnosis is patella cubiti (see 3.4.13).
f. Proximal radial fracture – uncommon; occasionally Salter–Harris type I fracture through the physis in young animals.
g. Monteggia fracture – uncommon; a proximal ulnar fracture (articular or non-articular) with cranial luxation of the radius and distal ulnar fragment.
18. Traumatic elbow luxation – usually due to a road traffic accident or suspension by the limb from a fence. ML radiographs may be almost normal, but the CrCd view shows dislocation of radius or ulna from humerus clearly; small avulsion or chip fractures may also be seen. Usually the radius and ulna luxate laterally as the large medial humeral epicondylar ridge prevents medial luxation. Ulnar luxation alone also reported.
19. Elbow osteoarthrosis (Fig. 3.11) – new bone mainly on the anconeus and radial head (seen on the ML view) and medial and lateral humeral epicondyles (seen on the CrCd view). Sclerosis of the ulnar trochlear notch is due to a combination of increased bone density and superimposition of osteophytes, and is seen especially in dogs with fragmented coronoid process. The lameness may be quite severe with mild radiographic changes.
a. Primary – ageing change; radiographic findings are usually minor.
b. Secondary – usually due to elbow dysplasia; radiographic findings may be severe.
3.5. RADIUS AND ULNA (ANTEBRACHIUM, FOREARM)
Views
ML; CrCd.
Development
Radius – the ossification centre of the diaphysis is present at birth; the proximal epiphysis appears at 3–5 weeks and fuses to the diaphysis at 5–11 months; the distal epiphysis appears at 2–4 weeks and fuses to the diaphysis at 6–12 months. Ulna – the ossification centre of the diaphysis is present at birth; the ossification centre of the anconeus appears at about 11–12 weeks and fuses to the olecranon at 3–5 months in large dogs; the olecranon appears at 8 weeks and fuses to the diaphysis at 5–10 months; the distal epiphysis appears at 2–4 weeks and fuses to the diaphysis at 6–12 months. The distal ulnar physis is conical in the dog, appearing V-shaped radiographically, and is flat and horizontal in the cat.
1. Late closure of the radial growth plates in neutered cats (males – distal only; females – both proximal and distal); leads to an overall longer radius than in entire cats.
2. Hemimelia (radial or ulnar agenesis) – one of the paired bones is congenitally absent, usually the radius; rare; usually unilateral. Medial carpal bones and the first digit may also be absent in the case of radial hemimelia; the remaining bone shows variable shape changes. Severe limb deformity and disability are evident from birth. Possibly heritable, as reported in several sibling cats.
3. Retained cartilaginous core, distal ulnar metaphysis (Fig. 3.12) – common, often bilateral, ossification defect in giant dog breeds, in which a central core of distal growth plate cartilage is slow to ossify, forming a candle flame-shaped lucency with faintly sclerotic borders. Implicated in growth disturbances but may be a coincidental finding, as often seen in normal dogs too.

4. Premature closure of the distal ulnar growth plate (radius curvus syndrome) (Fig. 3.13) – a common growth disturbance in young dogs of giant breeds, leading to angular limb deformity, often bilateral. The cause is usually not identified, so deemed idiopathic, but proposed mechanisms include:
a. Salter–Harris type V crush injury of the distal ulnar growth plate – susceptible to such injury due to its deep conical shape, which prevents lateral movement. May also occur unilaterally in other breeds.
b. Metaphyseal OC or retained cartilaginous core.

Radiographs should include the whole antebrachium including the elbow and carpus, and show shortening of the ulna and distraction of the lateral styloid process from the carpus, craniomedial bowing of the radius and ulna with thickening of the adjacent radial and ulnar cortices, carpal subluxation and remodelling of the distal radius, carpal valgus and external rotation of the foot, and secondary elbow subluxation, usually of the distal aspect of the humeroulnar articulation. Carpal valgus may also be due to distal radius or ulna fracture or to developmental laxity of the short radial collateral ligament, and radiography permits differentiation of these conditions.
5. Distractio cubiti or dysostosis enchondralis – asynchronous growth of the radius and ulna in chondrodystrophic breeds (e.g. Bassett Hound), leading to elbow incongruity and pain; widening of the distal aspect of the humeroulnar articulation. Usually present with elbow lameness at about 12 months of age; may be bilateral.
6. Premature closure of the distal radial growth plate – trauma at or near the growth plate causes reduction in growth of the radius with shortening of the bone and subluxation of the elbow; widening of the humeroradial articulation ± increased width of the humeroulnar space proximally. Angular limb deformity is usually minor, and the main clinical problem is elbow pain.
a. Symmetric closure – radius short and unusually straight, ulna may be slightly short too, elbow subluxation.
b. Asymmetric closure – distal radius remodelled.
– Lateral aspect (more common) – mimics premature closure of the distal ulnar growth plate with bowing of the radius and ulna and carpal valgus.
– Medial aspect – carpal varus.
7. Premature closure of the proximal radial growth plate – rare; presumed to be due to trauma; radiographic signs as for 6a, but the proximal radius may be obviously remodelled. Only 30% of the radial growth occurs proximally, therefore radial shortening is less severe than that following distal growth plate trauma.
8. Osteochondrodysplasias – various types of hereditary dwarfism are recognized in a number of dog breeds and in cats (see 1.22.7). Pathological and radiographic lesions are often most severe in the distal ulna and radius due to the high rate of growth at this site. The main abnormality is delayed growth at the distal ulnar growth plate, leading to shortening and bowing of the antebrachium. Some conditions may also resemble rickets radiographically (see 1.23.8 and Fig. 1.30). The pelvic limbs are less severely affected and may be normal.
9. Congenital hypothyroidism – causes dwarfism with radiographic changes similar to hereditary osteochondrodysplasias (see 1.22.9).
10. Radioulnar synostosis (fusion of the bones) leading to secondary radial head subluxation and external rotation of the foot has been described in a cat and is recognized in children. The radius and ulna are fused proximally at the interosseous space, preventing pronation–supination, and secondary elbow malformation results. May also occur following antebrachial fractures.
11. Bone remodelling in the distal ulnar and/or radial metaphyses has been described in Newfoundland dogs in Norway: 45% of dogs examined radiographically over a period of time showed islands of reduced opacity outlined by thickened trabeculae in the distal metaphyses at 6 months of age; the changes progressed up the diaphyses and persisted for up to 24 months of age. Aetiopathogenesis unclear. No clinical signs, but should not be mistaken for other conditions.
12. Metaphyseal osteopathy (syn. hypertrophic osteodystrophy) – young, rapidly growing dogs of larger breeds; lesions are usually most severe in the distal ulnar and radial metaphyses (see 1.24.4 and Fig. 1.31). Extensive periosteal and paracortical new bone may occasionally bridge growth plates, leading to angular limb deformities.
16. Craniomandibular osteopathy – rarely, paracortical new bone may be seen surrounding the distal ulna and radius, mimicking metaphyseal osteopathy (Fig. 3.14), sometimes in the absence of the typical skull lesions, although in dogs of appropriate breed and age (see 4.10.1 and Fig. 4.6).
17. Canine leucocyte adhesion deficiency – a hereditary, fatal disease in Irish Setters, causing lesions similar to metaphyseal osteopathy and craniomandibular osteopathy.
18. Primary malignant bone tumours (most commonly osteosarcoma) – the distal radial metaphysis is the main predilection site, especially in large and giant dog breeds, for example Great Dane, Irish Wolfhound (see 1.20.1 and Fig. 1.27).
21. Fractures of the antebrachium.
a. Transverse fracture of the radius and ulna is very common; usually distal one-third.
b. Fracture of one bone only occurs occasionally due to direct trauma.
c. Fissure fracture of the cranial cortex of the radius mid-shaft after jumping from a height has been reported.
d. Distal radial (medial styloid process) fractures usually occur as avulsion fractures of the short radial collateral ligaments and result in medial joint instability, detected on stressed radiographs.
e. Distal ulnar (lateral styloid process) fractures may be associated with damage to the origins of the short ulnar collateral ligaments and result in lateral joint instability, detected on stressed radiographs.
f. Avulsion of the origin of the dorsal radiocarpal ligament – racing Greyhounds; avulsion fragment from dorsomedial aspect of the distal radius.
3.6. CARPUS
Views
ML; flexed ML; dorsopalmar (DPa); dorsolateral–palmaromedial oblique; dorsomedial–palmarolateral oblique; stressed and weight-bearing views. Stressed views allow more accurate diagnosis of ligamentous injuries and should be obtained by using soft ties around the distal antebrachium and metacarpus and not by manual restraint. Oblique views of the carpus are helpful in interpretation, and similar radiographs of the normal leg for comparison are invaluable. On flexed ML radiographs, the antebrachiocarpal joint accounts for the majority of joint flexion, the middle carpal joint for some and the carpometacarpal joint for relatively little. The antebrachiocarpal joint normally also allows slight hyperextension.
Development
The ossification centres of the radial, ulnar and numbered carpal bones appear at 3–4 weeks; the body of the accessory carpal bone appears at 2 weeks and its epiphysis at 7 weeks, with fusion occurring at 10 weeks to 5 months.

1. Normal sesamoid in the insertion of abductor pollicis longus muscle on proximal metacarpal 1, seen on a DPa radiograph medial to the radial carpal bone; differential diagnosis is old chip fracture.
2. Developmental antebrachiocarpal subluxations – secondary to growth disturbances in the antebrachium and angular limb deformities; most commonly premature closure of the distal ulnar growth plate with cranial bowing of the radius, leading to articulation of the distal radius with the dorsoproximal margin of the radial carpal bone and remodelling of the distal radial epiphysis (see 3.5.4. and Fig. 3.13).
3. Carpal flexural deformity – skeletally immature dogs at about 6–12 weeks of age, especially the Dobermann. Thought to be due to relative shortening of flexor carpi ulnaris muscle. Radiographs are normal and are used to exclude bony pathology.
4. Cats – osteodystrophy of the Scottish Fold cat; changes are more severe in the pelvic limbs (see 3.7.8).
6. Cats – various feline polyarthritides; the carpus and tarsus are predilection sites.
7. Chinese Shar Pei fever syndrome, also known as familial renal amyloidosis of Chinese Shar Pei dogs – mainly the tarsus, but the carpus is occasionally affected (see 3.13.6).
8. Carpal fractures – often associated with avulsions of tendons or ligaments, so what appear to be minor fractures may cause serious effects.
Get Clinical Tree app for offline access
a. Accessory carpal bone fractures (Fig. 3.15) – especially racing Greyhounds and other athletic dogs; mainly the right carpus due to loading when running anticlockwise; best seen on extended and flexed ML radiographs. Five types are described:




– type 1 – accessoroulnar ligament avulsion from the base of the bone
– type 2 – avulsion of ligaments attaching to the radius and ulna, on the proximal border of the bone
– type 3 – avulsion of the origin of the accessorometacarpal ligaments
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree