Chapter 21 1. Ensuring that the duration of anesthesia is kept to a minimum commensurate with the performance of the procedure 2. Maintaining the mean arterial pressure >70 mmHg 3. The choice of suitable material for padding of the operating table surface The arterial partial pressure of oxygen is influenced by the size and position of the animal but is relatively uninfluenced by the respiratory depression associated with general anesthesia. Horses are likely to develop alveolar–arterial (A-a) gradients during general anesthesia, and these appear to be more marked with inhalational agents. A-a gradients occur when there is a difference between the oxygen tensions (pO2) in the lung alveoli (A) and the arterial circulation (a). A-a gradients are the result of a number of factors. The degree of A-a gradient does not appear to differ in those animals that breathe spontaneously compared to those that are subjected to intermittent positive pressure ventilation (IPPV). Factors that may contribute to the development of A-a gradients include pulmonary diffusion defects, progressive atelectasis, right to left intrapulmonary vascular shunts, redistribution of pulmonary blood flow relative to ventilation and a reduction in cardiac output without a reduction in tissue oxygen consumption. General bodily condition should be considered as obesity can influence respiratory movements, and both obesity and extreme thinness may interfere with the disposition of drugs in the body. A history of recent trauma should be thoroughly investigated and during physical examination special attention should be directed to the possible presence of such common conditions as diaphragmatic or bladder rupture and to hemorrhage. Hemorrhage, particularly when it is from the nose or associated with trauma and accompanied by tachycardia, will suggest that it is severe and usually will necessitate treatment with circulatory blood volume expanders (q.v.). Horses should be weighed wherever possible but formulae and tape measures may be used in the absence of a weigh scales and provide a reasonably accurate estimate of a horse’s weight. (See also page 173.) A number of drugs are available for the purposes of premedication, sedation and restraint but, as there is some confusion over the terminology used to describe the various classes of drugs and their effects in horses, the following definitions are used here. A hypnotic depresses the central nervous system and tends to produce sleep; these agents are rarely used in horses. A sedative is a drug that relieves anxiety and produces a state of drowsiness. Many drugs appear to be both hypnotic and sedative with dose related effects. Chloral hydrate and xylazine are typical examples in the horse. A tranquilizer or ataractic drug is one that relieves anxiety and produces a variable degree of sedation. Three categories of tranquilizer are described: hypnotic/sedatives, antipsychotics and anxiolytics. Benzodiazepines are both anxiolytics and sedative/hypnotics. Antipsychotics are also known as neuroleptics and are typified by the butyrophenones and the phenothiazines. Four main groups of drugs are used to premedicate and sedate horses ( Box 21.1). These are phenothiazines, benzodiazepines, α2-adrenoceptor agonists and anticholinergics. ACP produces muscular relaxation, which appears more marked when it is given IV. In males this produces relaxation of the retractor penis muscle and hence protrusion of the penis. The penis is normally flaccid but there have been a few reports of priapism (sustained erection) (q.v.). Penile protrusion is normally of short duration but if it is prolonged it should be treated by massage, compression and lubrication. It is extremely important to avoid damage to the penis, and support should be provided to keep the penis as close to the body wall as possible.
Anesthesiology
GENERAL CONSIDERATIONS IN ANESTHETIZING HORSES
PREPARATION FOR GENERAL ANESTHESIA
PREMEDICATION, SEDATION AND CHEMICAL RESTRAINT
DEFINITIONS
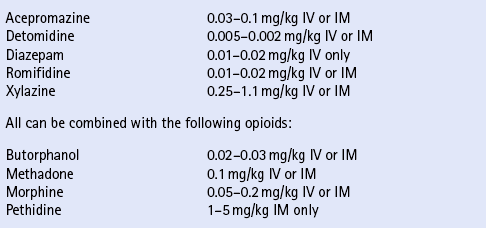
PHENOTHIAZINES
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


