Figure 36.2 Postmortem photograph of specimen in left lateral recumbency to view approximate orientation of viscera viewed through the right abdomen. The twelfth rib (A), the diaphragm (B), C-3 (C), and saccules of C-1 (D), are shown.
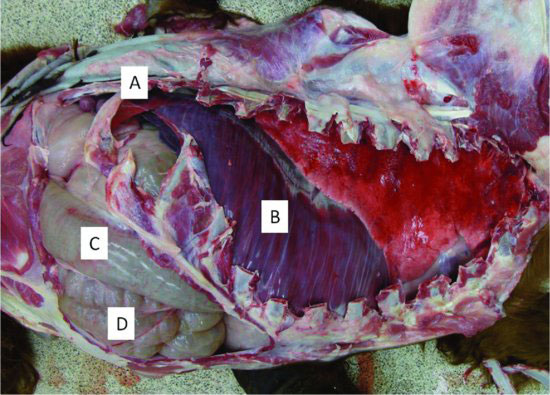
Figure 36.3 Postmortem photograph of specimen in left lateral recumbency showing orientation of C-3 and duodenum. The glandular portion of C-3 (A), the nonglandular C-3 (B), and the proximal portion of the duodenum (C), are shown. The liver is labeled (D).
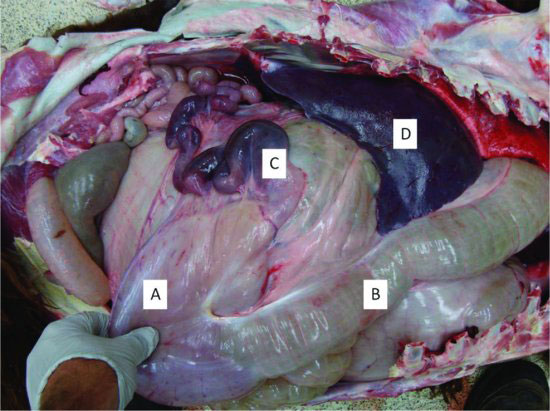
The small intestinal tract courses along to fill the right ventral quadrant of the abdomen. The duodenum exits the pylorus of C-3 (See Figure 36.3.), where a prominent ampulla, or luminal dilatation, is present. This normal duodenal dilatation has been mistaken for pathologic dilatation, diverticula, or stricture. The duodenum first courses cranial-dorsal to the liver before returning distal to the jejunum then finally transitioning into the ileum, which terminates in the ceco-colic orifice in the central abdomen. Camelids do not have a distinct ileocecal junction or ceco-colic junction.
The large intestinal tract consists of a cecum, proximal ascending colon, spiral-ascending colon, distal ascending colon, transverse colon, descending colon, and rectum. The apex of the cecum is directed caudally toward the pelvis, followed by a long proximal loop of ascending colon entering a tighter spiral colon situated in the mid to ventral abdomen. Feces exit by way of the distal loop of the ascending colon into the transverse colon (right to left), descending colon, rectum, and anus. The duodenum and pylorus are common sites for trichobezoars to become lodged and cause obstruction. The spiral colon is a common site for fecaliths to become lodged and cause obstruction of the flexure of the central loop. The elongated proximal loop of the ascending colon may become displaced causing impaction or obstruction.
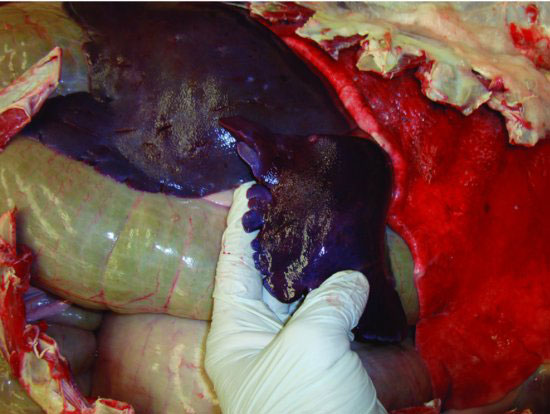
The anatomic association of the llama liver has recently been investigated (Castro et al., 2009). The liver is situated in the right cranial abdomen. (See Figure 36.3.) The caudo-dorsal border is at the level of the twelfth rib and the caudo-ventral border extends to about the fifth or sixth rib, covering C-2 and all but a small ventral portion of C-3. The liver is a solid, lobulated organ, and the caudal border may appear rough or fimbriated. (See Figure 36.4.) Camelids do not have a gall bladder, but dilatations of the bile duct have been observed during necropsy in rare cases.
Figure 36.4 The edge of the liver margin may appear irregular or fimbriated and is considered normal.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


