Figure 38.2 The depression of the linea alba can be palpated just caudal or cranial to the umbilicus.

For paracostal or midline abdominocentesis utilizing a teat cannula, clip and surgically prep the skin over the area to be aspirated. Inject 2 to 3 mL of 2% lidocaine subcutaneously and into the soft tissues. A small (0.5-cm) stab incision is made with the #15 scalpel blade through the skin only. (See Figure 38.3.) Insert the teat cannula perpendicular to the body wall and through the soft tissues and the peritoneum. (See Figure 38.4.) A firm thrust is necessary to penetrate the peritoneum, and the operator will sense a sudden release of pressure. Peritoneal fluid may flow freely, and adjustments of depth and rotation of the cannula may facilitate flow. (See Figure 38.5.) Care must be taken not to introduce the cannula into a distended viscus. For this reason, ultrasonographic examination of the target region is encouraged immediately prior to insertion of the cannula. After collecting the sample, remove the teat cannula. The small stab incision may be left to heal by second intention, or a single skin suture or skin staple may be placed.
Figure 38.3 A #15 scalpel blade is used to make a stab incision through the skin when utilizing a teat cannula for abdominocentesis.

Figure 38.4 A teat cannula is inserted through the stab skin incision and the deeper soft tissues perpendicular to the abdominal wall. A quick thrust is necessary to penetrate the peritoneum.

Figure 38.5 Peritoneal fluid is seen flowing from the teat cannula in this image, and could be collected in a suitable container for analysis.

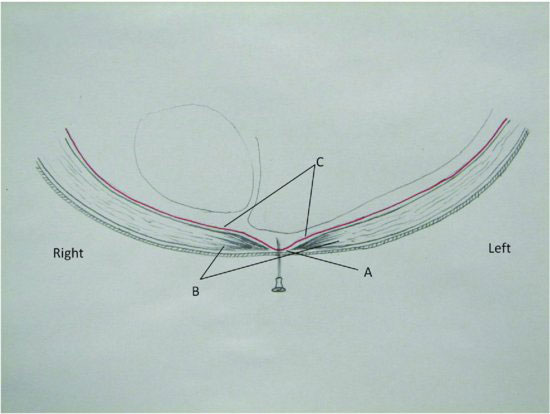
Alternatively, an 18-gauge hypodermic needle may be used for collection of peritoneal fluid at the midline location. The abdominal muscles, peritoneum, and soft tissues converge at the linea and provide a natural trough for fluid accumulation. (See Figure 38.6.) Llamas and alpacas deposit considerable fat into the retroperitoneal space. This “fat pad” often interferes with paramedian attempts to obtain abdominal fluid. The attachment of the peritoneum to the linea alba creates a window of access free of this fat interference. The anatomical trough that is created is most prominent cranial to the umbilicus and tapers considerably caudal to the umbilicus.
Figure 38.6 Cross-sectional abdominal diagram viewed from cranial to caudal. Linea alba (A), abdominal musculature (B), peritoneum (C). A natural linear depression (trough) is formed where the abdominal musculature and soft tissues converge at the linea alba. Peritoneal fluid can be collected with a hypodermic needle.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


