Figure 37.2 The probe is placed in the dorsal portion of the tenth intercostal space then moved ventrally.


Continue imaging the right ventral quadrant of the abdomen to view the small bowel. Motility patterns and ultrasonographic appearance of the small bowel in normal camelids have been described (Cebra et al., 2002). The right paralumbar area will produce images of the ascending colon and large bowel. Segments of small bowel have a more hypoechoic intraluminal ingesta and more frequent motility patterns than large intestinal segments. Nonmotile, distended loops of small intestine, possibly with a plicated appearance and containing static ingesta, are indicative of obstruction. Ultrasound guided abdominocentesis can be performed to collect and analyze peritoneal fluid. This must be done cautiously in cases with significant distention of intestines or forestomach compartments. Aside from ascites and uroabdomen, Streptococcus zooepidemicus infection has been noted to result in significant peritoneal effusion (Jones et al., 2009; Hewson et al., 2001).
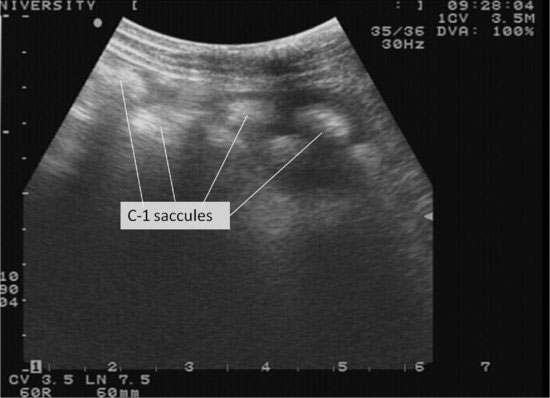
The ventral surface of the cranial and caudal portions of the first compartment can be imaged via the left ventral abdomen. Compartment motility can be evaluated, however, due to the glandular saccules and orientation of the compartment, ingesta consistency is not able to be defined unless there has been profound dissipation of the fiber content and reduction of gas production. The saccules have a characteristic appearance to orient the clinician on position within the abdomen. (See Figure 37.6.) Small volumes of free peritoneal fluid may be seen in this area.
Figure 37.6 An ultrasound image of the left ventral abdomen just caudal to the xyphoid showing the appearance of the saccules of the first compartment.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


