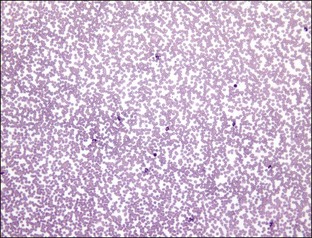
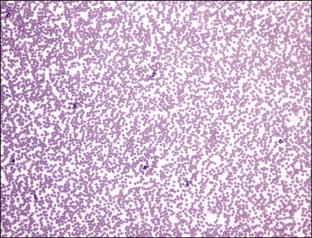
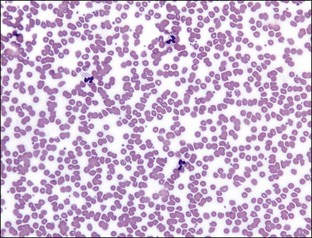
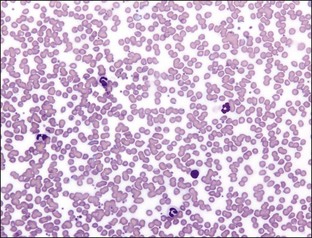
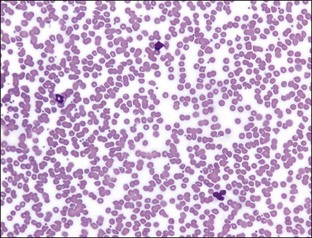
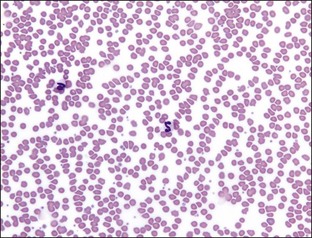
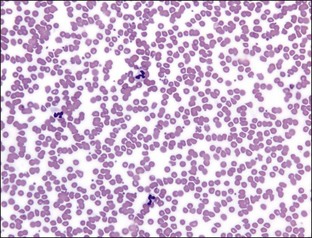
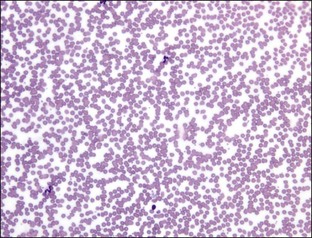
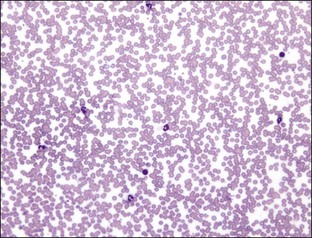
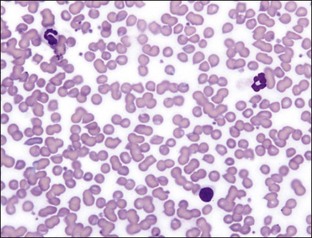
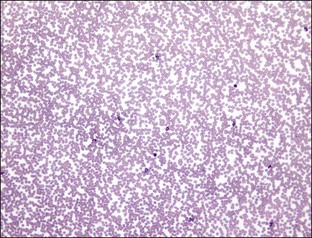
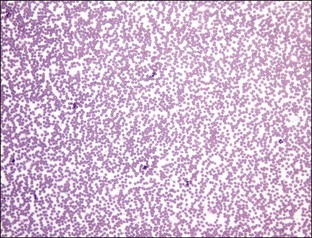
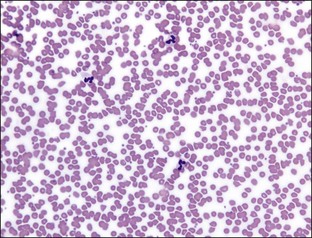
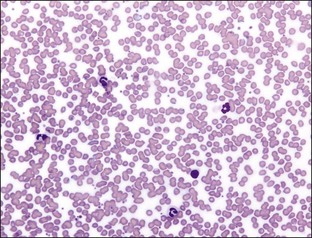
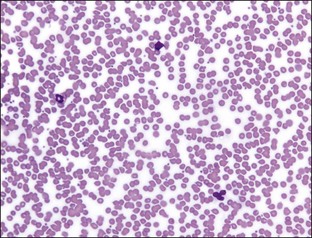
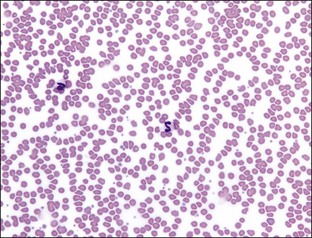
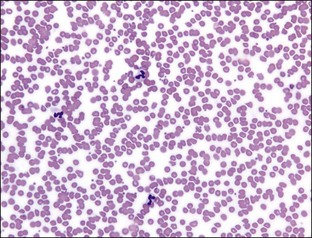
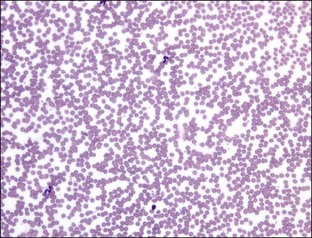
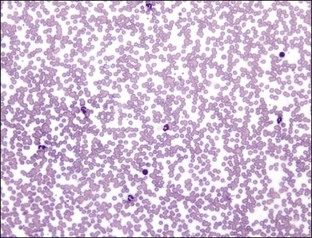
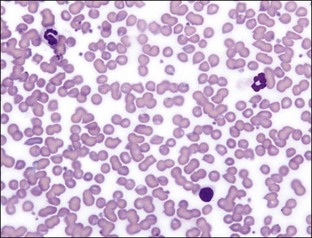
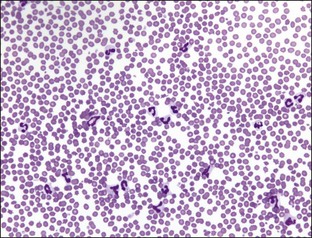
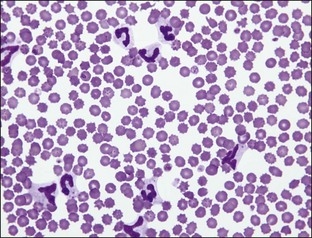
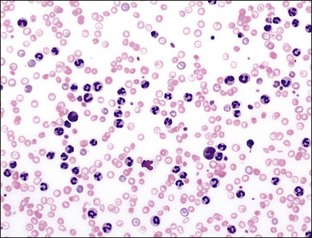
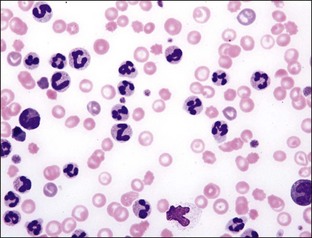
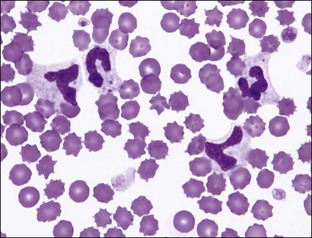
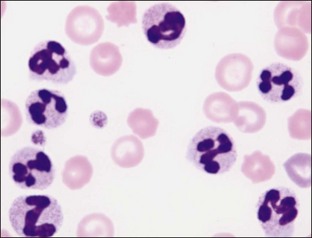
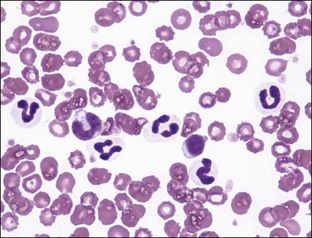
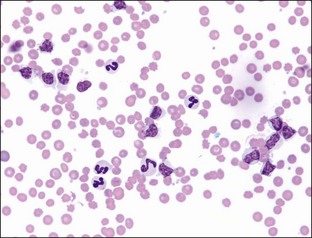
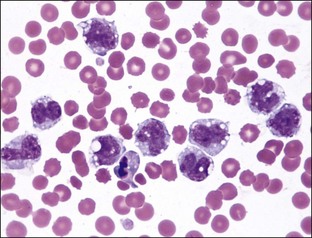
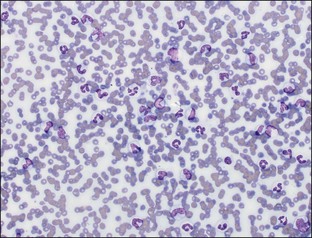
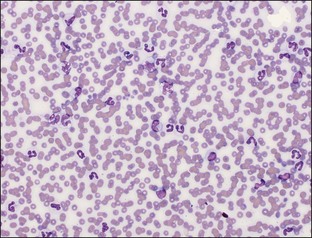
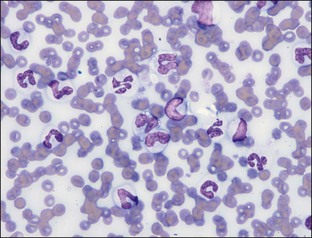
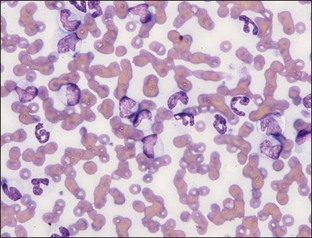
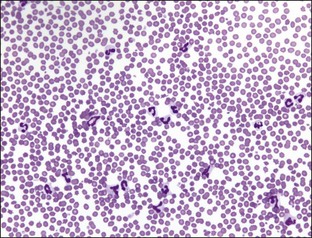
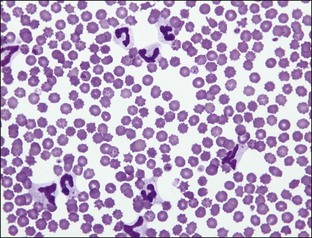
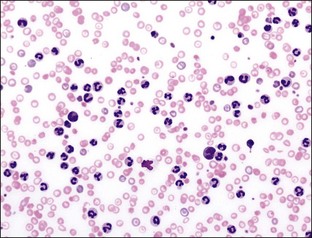
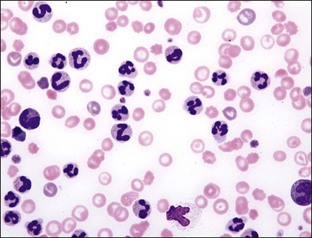
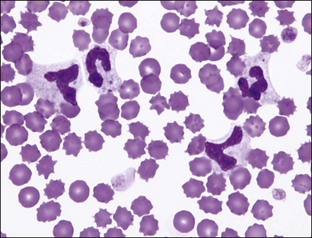
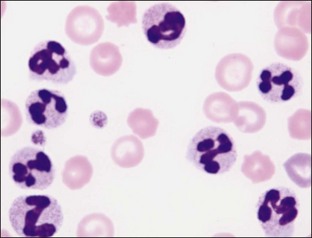
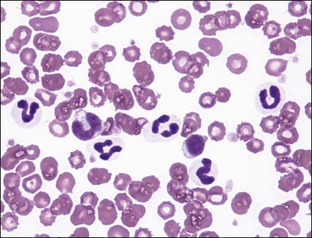
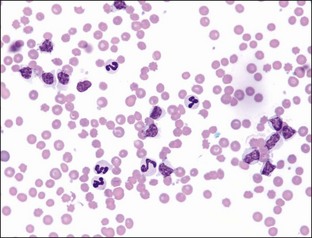
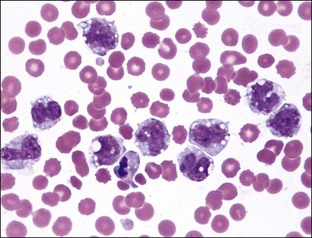
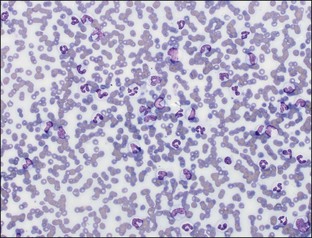
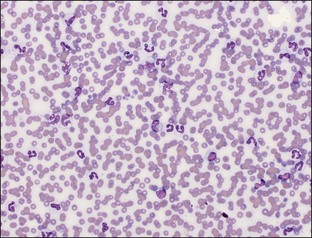
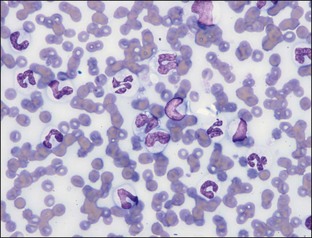
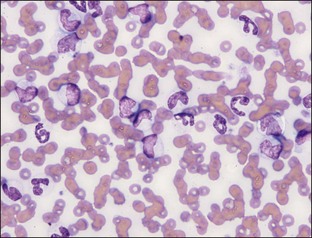
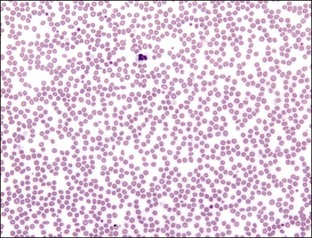
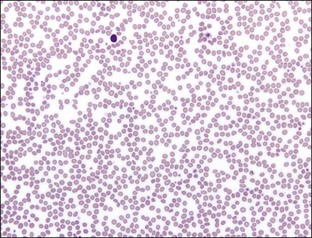
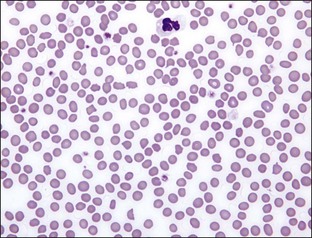
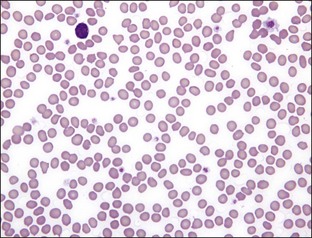
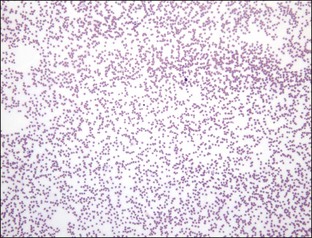
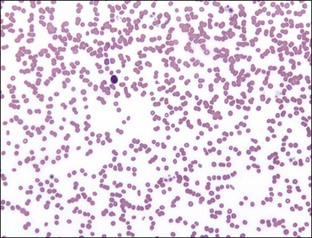
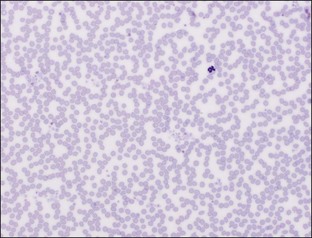
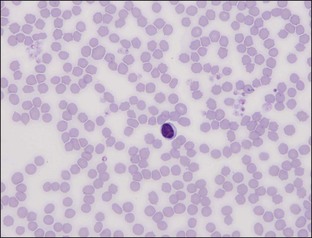
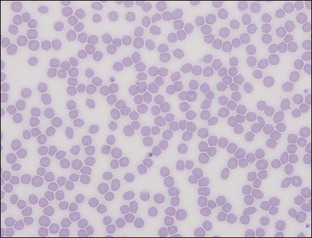
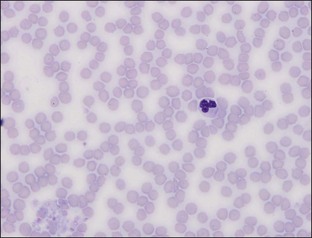
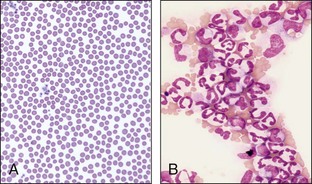
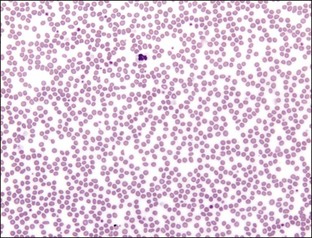
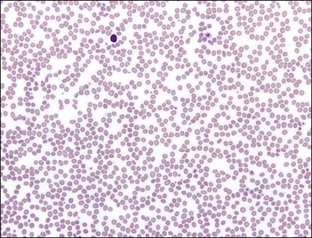
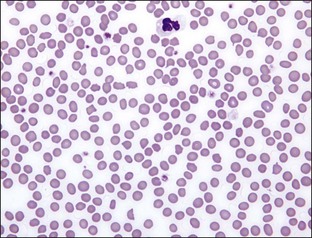
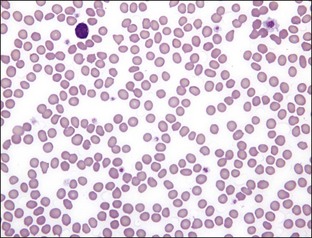
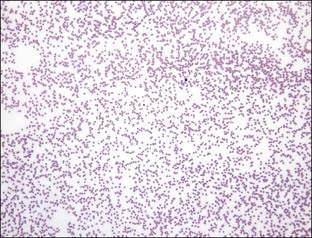
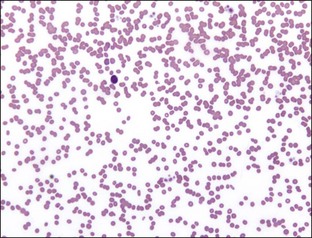
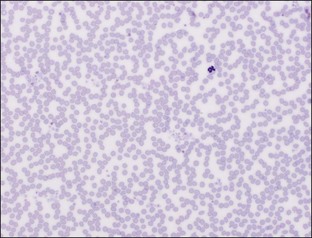
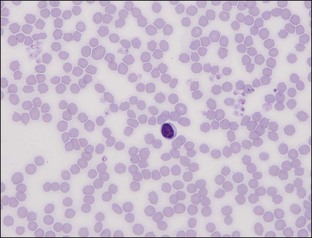
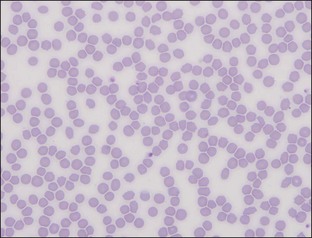
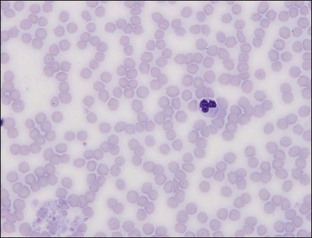
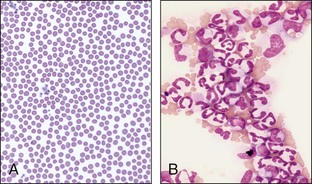
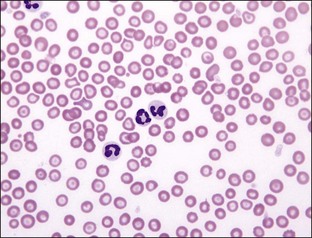
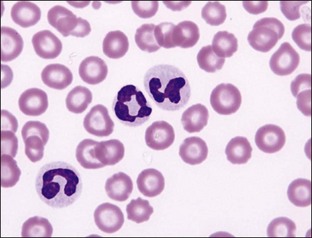
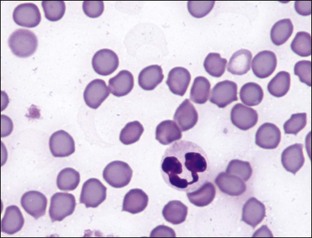
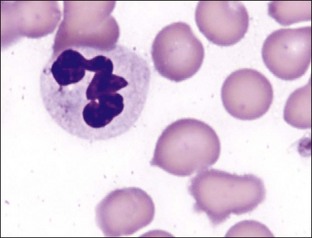
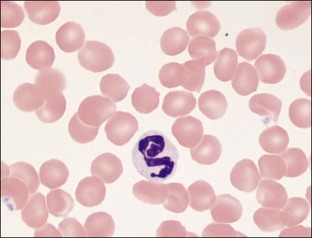
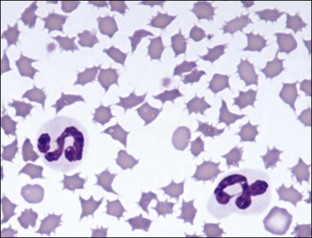
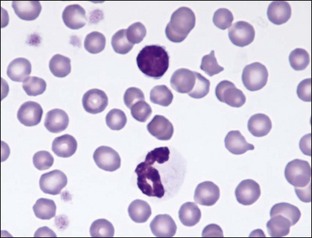
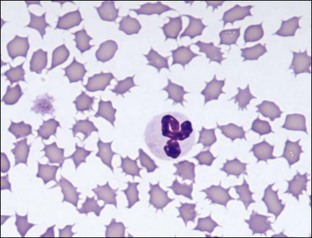
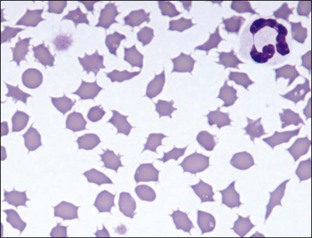
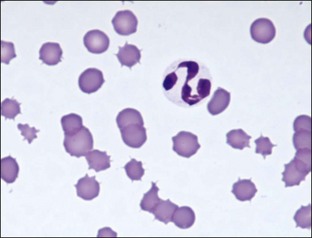
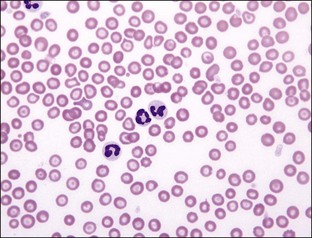
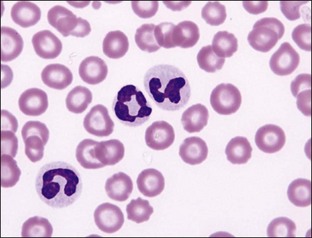
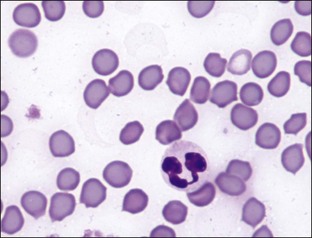
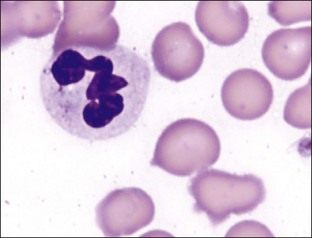
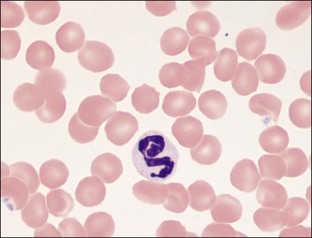
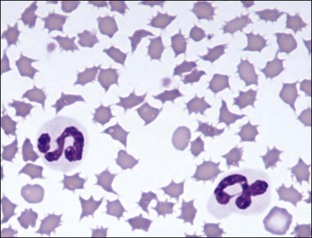
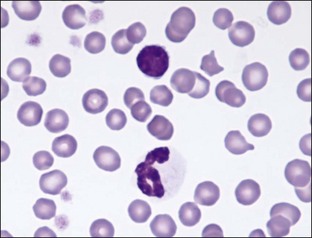
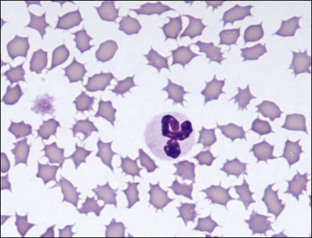
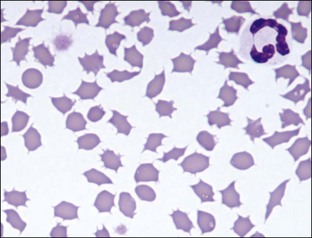
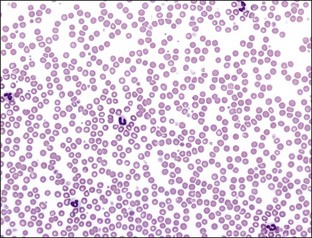
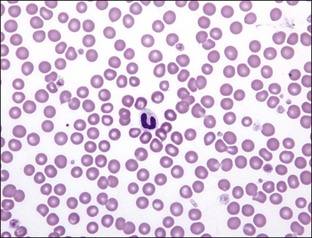
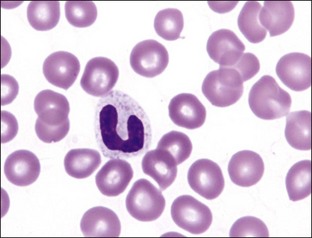
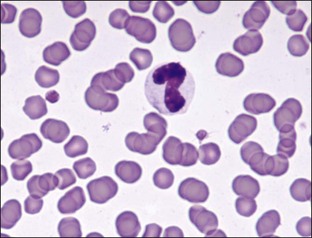
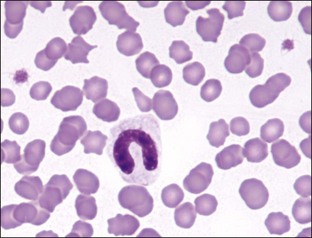
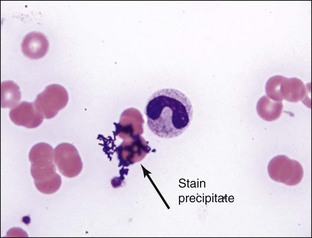
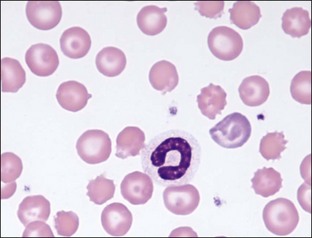
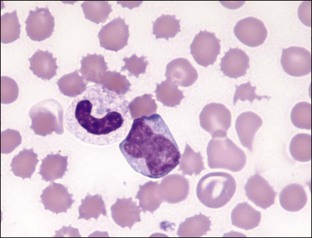
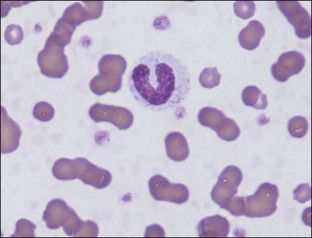
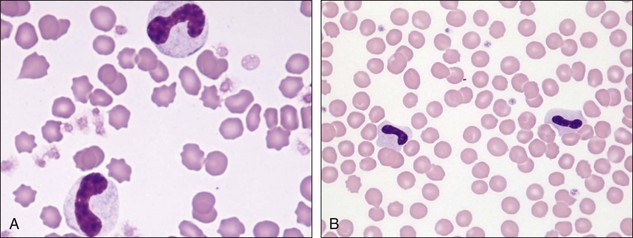
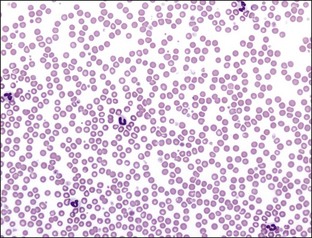
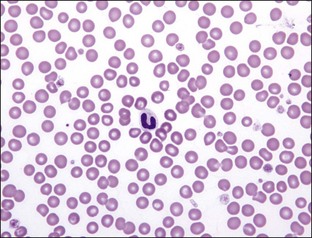
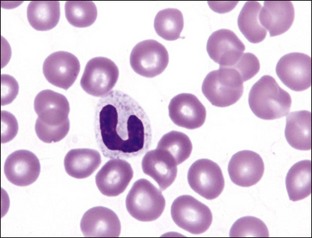
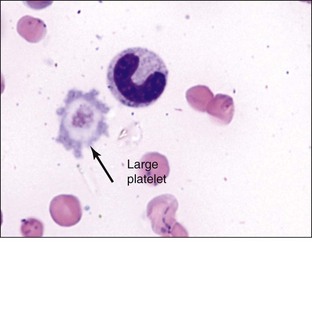
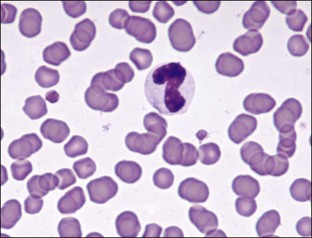
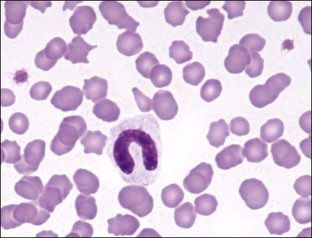
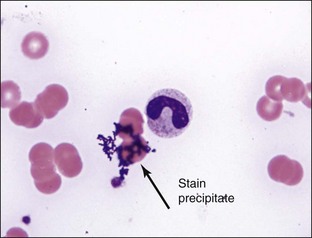
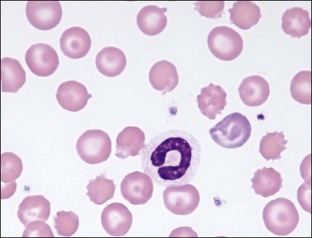
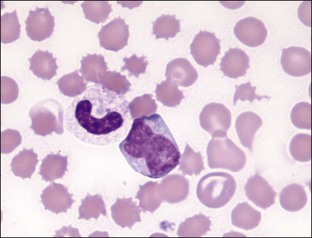
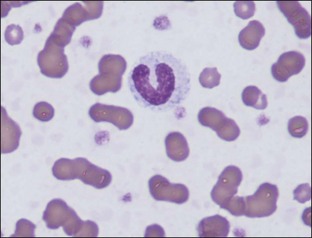
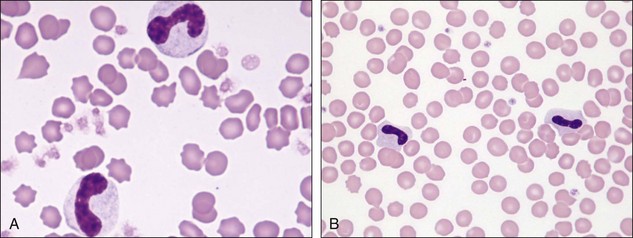
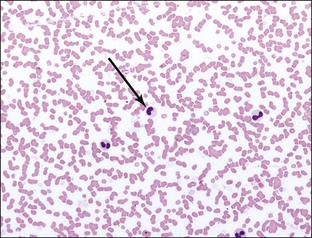
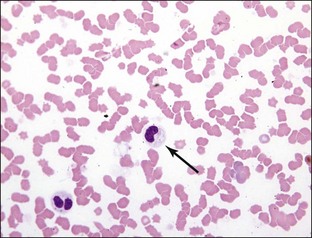
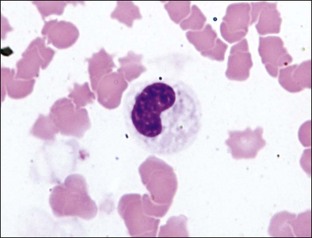
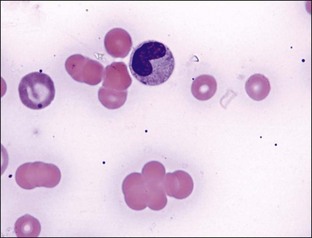
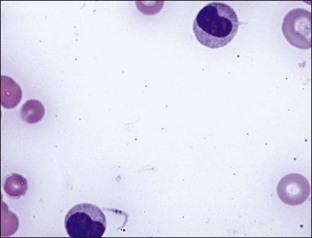
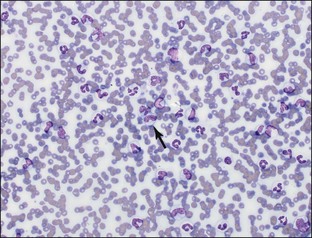
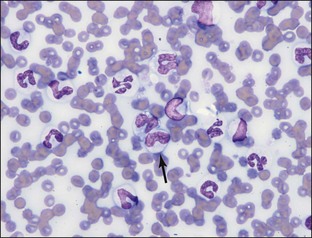
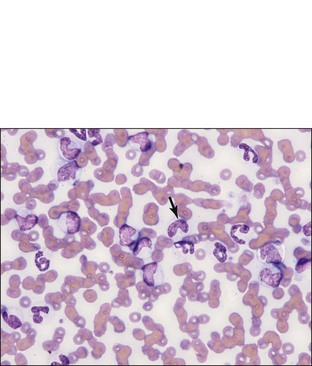
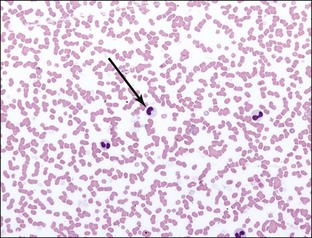
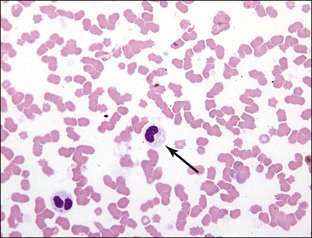
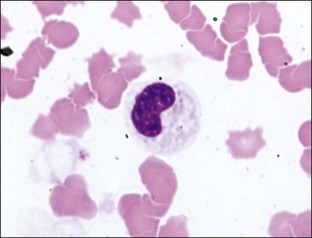
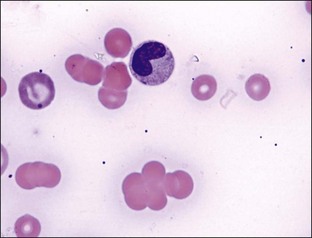
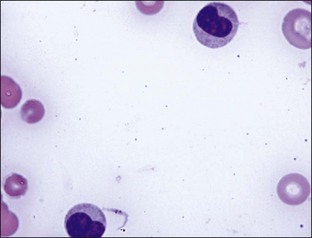
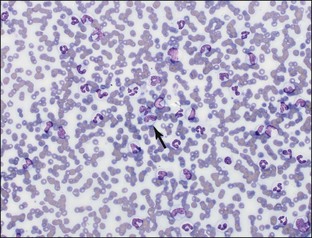
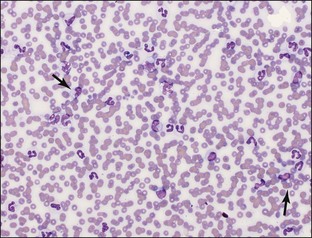
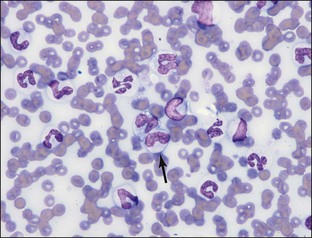
Section 3 White Blood Cells Normal Leukocyte Count Leukocytosis Leukopenia Neutrophils Mature (Segmented) Neutrophils Band Neutrophils Metamyelocytes Myelocytes Promyelocytes Myeloblasts Barr Body Hypersegmented Neutrophils Pelger-Huët and Pseudo-Pelger-Huët Neutrophils Toxic Changes Döhle Bodies Diffuse Cytoplasmic Basophilia Cytoplasmic Vacuolization (Foamy Cytoplasm) Toxic Granulation Ring (Doughnut) Form Giant Neutrophils Lymphocytes Small Lymphocytes Reactive Lymphocytes Plasmacytoid Reactive Lymphocytes Granular Lymphocytes (Large Granular Lymphocytes) Monocytes Eosinophils Basophils Mast Cells Sideroleukocytes Erythrophage (Erythrophagocytosis) Macrophage Inclusions, Parasites, and Infectious Agents Distemper Inclusions Ehrlichia/Anaplasma spp. Hepatozoon spp. Histoplasma capsulatum Mucopolysaccharidosis Chédiak-Higashi Syndrome Birman Cat Anomaly GM Gangliosidosis White Blood Cell Artifacts Pyknotic Cells Basket or Smudge Cells Platelet over White Blood Cell Changes Associated with Delayed Processing Understained Smears Normal Leukocyte Count Diagnostic Significance: A scan of the blood film may determine relative numbers of blood leukocytes and may be used to provide quality control of complete blood count (CBC) results obtained by hematology analyzers. The presence of normal numbers of leukocytes does not rule out disease of infectious, inflammatory, or neoplastic origin, emphasizing the need for careful microscopic review of cellular morphology. Plate 3-1 Normal Leukocyte Count Next Topic Plate 3-1a Plate 3-1b Plate 3-1c Plate 3-1d Plate 3-1e Plate 3-1f Plate 3-1g Plate 3-1h Plate 3-1i Plate 3-1j Plate 3-1a Return to text. Return to image plate. Plate 3-1b Return to text. Return to image plate. Plate 3-1c Return to text. Return to image plate. Plate 3-1d Return to text. Return to image plate. Plate 3-1e Return to text. Return to image plate. Plate 3-1f Return to text. Return to image plate. Plate 3-1g Return to text. Return to image plate. Plate 3-1h Return to text. Return to image plate. Plate 3-1i Return to text. Return to image plate. Plate 3-1j Return to text. Return to image plate. Leukocytosis Diagnostic Significance: Leukocytosis is defined as the presence of increased leukocyte numbers, which may be caused by an increase in the number of one cell type or a combination of cell types. The significance of a leukocytosis is based on the degree of elevation, the cell types constituting the increase, and the cellular morphology (normal, dysplastic, toxic, neoplastic). Increased numbers of neutrophils secondary to inflammation is the most common cause of a leukocytosis. Plate 3-2 Leukocytosis Next Topic Plate 3-2a Plate 3-2b Plate 3-2c Plate 3-2d Plate 3-2e Plate 3-2f Plate 3-2g Plate 3-2h Plate 3-2i Plate 3-2k Plate 3-2l Plate 3-2m Plate 3-2n Plate 3-2a Return to text. Return to image plate. Plate 3-2b Return to text. Return to image plate. Plate 3-2c Return to text. Return to image plate. Plate 3-2d Return to text. Return to image plate. Plate 3-2e Return to text. Return to image plate. Plate 3-2f Return to text. Return to image plate. Plate 3-2g Return to text. Return to image plate. Plate 3-2h Return to text. Return to image plate. Plate 3-2i Return to text. Return to image plate. Plate 3-2k Return to text. Return to image plate. Plate 3-2l Return to text. Return to image plate. Plate 3-2m Return to text. Return to image plate. Plate 3-2n Return to text. Return to image plate. Leukopenia Diagnostic Significance: Leukopenia is defined as a decrease in leukocyte numbers, which is most often caused by a decrease in the number of neutrophils (neutropenia), as neutrophils are the most numerous of the peripheral blood leukocytes. Careful exam of the entire blood smear is emphasized by the fact that sometimes during blood smear preparation, the leukocytes can be concentrated on the feathered edge. In this case, the monolayer will contain very few leukocytes, suggesting an artifactual leukopenia if the monolayer only, and not the entire slide, is examined for WBC estimation. Plate 3-3 Leukopenia Artifactual leukopenia. A, Monolayer, devoid of leukocytes B, Same smear where leukocytes are concentrated on the feathered edge Next Topic Plate 3-3a Plate 3-3b Plate 3-3c Plate 3-3d Plate 3-3e Plate 3-3f Plate 3-3g Plate 3-3h Plate 3-3i Plate 3-3j Plate 3-3a Return to text. Return to image plate. Plate 3-3b Return to text. Return to image plate. Plate 3-3c Return to text. Return to image plate. Plate 3-3d Return to text. Return to image plate. Plate 3-3e Return to text. Return to image plate. Plate 3-3f Return to text. Return to image plate. Plate 3-3g Return to text. Return to image plate. Plate 3-3h Return to text. Return to image plate. Plate 3-3i Return to text. Return to image plate. Plate 3-3j Return to text. Return to image plate. Return to text. Return to image plate. Neutrophils Neutrophils are the most abundant of the granulocytic cell types. Maturation stages from least mature to most mature are: myeloblasts, promyelocytes, myelocytes, metamyelocytes, band neutrophils, and mature (segmented) neutrophils. As cells mature, they decrease in size, the cytoplasm becomes less blue and eventually becomes clear to lightly colored, and the nucleus becomes more condensed and eventually lobulated. Neutrophils are released from bone marrow into circulation in an age-related fashion, with the most mature cells (mature neutrophils) released first. The bone marrow has a storage pool of mature neutrophils, so immature forms are not released into the circulation until the demand (severe, acute infection and inflammation) for neutrophils exceeds the storage pool’s ability to supply adequate numbers of mature cells. Increased numbers of immature neutrophils in the peripheral blood is referred to as a “left shift” and is the hallmark of acute inflammation. Immature neutrophils are also released in an age-related fashion, and as such, the immature neutrophil stage primarily seen in peripheral blood during a left shift is the band neutrophil, with less mature stages seen only rarely. In general, the more severe the systemic inflammation, the higher the number of neutrophils with increased numbers of immature forms present. The morphology and diagnostic significance of the various neutrophil maturational stages and the abnormalities that occur in the neutrophil series are discussed below. Mature (Segmented) Neutrophils Distinctive Features: Mature neutrophils of dogs and cats have similar morphologies. Neutrophils are round and approximately 10 to 12 micrometers (µm) in diameter. The cytoplasm is clear, moderately abundant, and may contain a few very indistinct, faint pink granules, and/or small clear vacuoles, or both. The nucleus is highly condensed and lobulated, generally containing three or four lobules. Nuclear lobes may be connected by a thin strand of chromatin, but more commonly, simply a narrowing of the chromatin exists between lobes to about one third the diameter of the thick portion of the lobules. Diagnostic Significance: Mature neutrophil numbers are increased (neutrophilia) in conditions such as epinephrine release (from excitement), endogenous steroids (stress resulting in glucocorticoid release), steroid administration, inflammation (infectious and noninfectious causes), tissue necrosis, and neoplasia. Mature neutrophilia caused by inflammation is often associated with an increase in band neutrophils (left shift). Leukemoid response is a term used to describe a marked neutrophilia, often with a left shift, which may be seen with severe, acute, focal inflammation (i.e., pyometra, peritonitis, pyothorax, severe abscessation). A persistently increasing, moderate to marked neutrophilia, in which a source of inflammation, infection, tissue destruction, or necrosis cannot be found, should raise the suspicion for chronic granulocytic leukemia. Mature neutrophil numbers are decreased (neutropenia) by conditions such as overwhelming bacterial infections, viral infections (parvovirus, panleukopenia, feline leukemia virus [FeLV]), certain bacterial infections (Salmonella), rickettsial infections (i.e., chronic ehrlichiosis), endotoxemia (infection with gram-negative bacteria), chemotherapeutic agents, bone marrow necrosis, myelophthesic diseases (bone marrow infiltration with neoplastic cells), and bone marrow suppression or failure (i.e., drug-induced neutropenia, immune-mediated neutropenia, cyclic hematopoiesis). Plate 3-4 Normal Mature Segmented Neutrophils Next Topic Plate 3-4a Plate 3-4b Plate 3-4c Plate 3-4d Plate 3-4e Plate 3-4f Plate 3-4g Plate 3-4h Plate 3-4i Plate 3-4j Plate 3-4a Return to text. Return to image plate. Plate 3-4b Return to text. Return to image plate. Plate 3-4c Return to text. Return to image plate. Plate 3-4d Return to text. Return to image plate. Plate 3-4e Return to text. Return to image plate. Plate 3-4f Return to text. Return to image plate. Plate 3-4g Return to text. Return to image plate. Plate 3-4h Return to text. Return to image plate. Plate 3-4i Return to text. Return to image plate. Plate 3-4j Return to text. Return to image plate. Band Neutrophils Distinctive Features: Band neutrophils are similar in size and appearance to mature neutrophils except that the nuclei are nonsegmented (band shaped) or only slightly constricted, and nuclear chromatin is not as tightly clumped. The classic band neutrophil has a plump C-shaped or S-shaped nucleus, with parallel sides, a smooth nuclear margin, and a fairly constant width. If slight constricted areas are present, they are more than one third the width of the rest of the nucleus, distinguishing the bands from mature neutrophils, which have constricted areas of less than one third the width of other areas of the nucleus. The nuclear chromatin is less dense than that of a mature neutrophil. The cytoplasm remains clear unless toxic change is present. Diagnostic Significance: Band neutrophils are either absent or present in very low numbers in healthy dogs and cats. A left shift is the hallmark of acute inflammation. Systemic inflammatory mediators travel to bone marrow, resulting in the production and release of neutrophils. Despite this systemic response, the inflammation may be focal (i.e., pyometra) or diffuse (i.e., bacterial sepsis). Additionally, not all focal areas of inflammation induce a systemic response. For example, cystitis (inflammation of the bladder) is not generally associated with an increased number of band neutrophils. Chronic granulocytic leukemia may also cause an increase in band neutrophil numbers. Also, pseudo–band neutrophils (hyposegmented mature neutrophils) may be seen in Pelger-Huët anomaly (discussed later). A left shift may be regenerative or degenerative. A regenerative left shift is a predominance of mature neutrophils (neutrophilia) with fewer bands, indicating a normal response to inflammation. A degenerative left shift occurs when bands (and often more immature forms of neutrophils) exceed the number of mature neutrophils. Often, a concurrent neutropenia exists. This indicates neutrophil production is not able to meet demand and is associated with a guarded or poor prognosis. Toxic changes are frequent with degenerative left shifts. As band neutrophils are the most common immature neutrophil released into peripheral blood and cannot be distinguished from mature neutrophils with current hematology analyzers, blood smear evaluation is extremely important in identifying and quantitating a left shift. Plate 3-5 Band Neutrophils A, Band neutrophils. Note the open chromatin B, Neutrophils with Pelger-Huët Anomaly. Note the condensed chromatin Next Topic Plate 3-5a Plate 3-5b Plate 3-5c Plate 3-5d Plate 3-5e Plate 3-5f Plate 3-5g Plate 3-5h Plate 3-5i Plate 3-5j Plate 3-5a Return to text. Return to image plate. Plate 3-5b Return to text. Return to image plate. Plate 3-5c Return to text. Return to image plate. Plate 3-5d Return to text. Return to image plate. Plate 3-5e Return to text. Return to image plate. Plate 3-5f Return to text. Return to image plate. Plate 3-5g Return to text. Return to image plate. Plate 3-5h Return to text. Return to image plate. Plate 3-5i Return to text. Return to image plate. Plate 3-5j Return to text. Return to image plate. Return to text. Return to image plate. Metamyelocytes Distinctive Features: Metamyelocytes are about the same size to slightly larger than mature and band neutrophils. The nuclei have one margin indented more than 25% into the nucleus and have an indented or kidney-shaped nucleus. The nuclear chromatin is readily recognized as condensed but generally less so than that of band neutrophils. The cytoplasm is nearly colorless but more basophilic than the nontoxic band neutrophil. Diagnostic Significance: Metamyelocytes are rarely seen in the peripheral blood of healthy dogs and cats. Metamyelocytes are sometimes seen in peripheral blood during severe inflammation along with band neutrophils as part of a left shift. Granulocytic leukemia may also cause an increase in metamyelocytes but occurs rarely. Also, pseudometamyelocytes (hyposegmented mature neutrophils) may be seen in Pelger-Huët anomaly (discussed later). Plate 3-6 Metamyelocytes Next Topic Plate 3-6a Plate 3-6b Plate 3-6c Plate 3-6d Plate 3-6e Plate 3-6f Plate 3-6g Plate 3-6h Plate 3-6i Plate 3-6j Plate 3-6a Return to text. Return to image plate. Plate 3-6b Return to text. Return to image plate. Plate 3-6c Return to text. Return to image plate. Plate 3-6d Return to text. Return to image plate. Plate 3-6e Return to text. Return to image plate. Plate 3-6f Return to text. Return to image plate. Plate 3-6g Return to text. Return to image plate. Plate 3-6h Return to text. Return to image plate. Plate 3-6i Return to text. Return to image plate.< div class='tao-gold-member'> Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Related Related posts: 6: Extracellular Organisms 4: Platelets 1: General Assessment 5: Hematopoietic Neoplasia Stay updated, free articles. Join our Telegram channel Join Tags: Atlas of Canine and Feline Peripheral Blood Smears Jul 24, 2016 | Posted by admin in SMALL ANIMAL | Comments Off on 3: White Blood Cells Full access? Get Clinical Tree
Section 3 White Blood Cells Normal Leukocyte Count Leukocytosis Leukopenia Neutrophils Mature (Segmented) Neutrophils Band Neutrophils Metamyelocytes Myelocytes Promyelocytes Myeloblasts Barr Body Hypersegmented Neutrophils Pelger-Huët and Pseudo-Pelger-Huët Neutrophils Toxic Changes Döhle Bodies Diffuse Cytoplasmic Basophilia Cytoplasmic Vacuolization (Foamy Cytoplasm) Toxic Granulation Ring (Doughnut) Form Giant Neutrophils Lymphocytes Small Lymphocytes Reactive Lymphocytes Plasmacytoid Reactive Lymphocytes Granular Lymphocytes (Large Granular Lymphocytes) Monocytes Eosinophils Basophils Mast Cells Sideroleukocytes Erythrophage (Erythrophagocytosis) Macrophage Inclusions, Parasites, and Infectious Agents Distemper Inclusions Ehrlichia/Anaplasma spp. Hepatozoon spp. Histoplasma capsulatum Mucopolysaccharidosis Chédiak-Higashi Syndrome Birman Cat Anomaly GM Gangliosidosis White Blood Cell Artifacts Pyknotic Cells Basket or Smudge Cells Platelet over White Blood Cell Changes Associated with Delayed Processing Understained Smears Normal Leukocyte Count Diagnostic Significance: A scan of the blood film may determine relative numbers of blood leukocytes and may be used to provide quality control of complete blood count (CBC) results obtained by hematology analyzers. The presence of normal numbers of leukocytes does not rule out disease of infectious, inflammatory, or neoplastic origin, emphasizing the need for careful microscopic review of cellular morphology. Plate 3-1 Normal Leukocyte Count Next Topic Plate 3-1a Plate 3-1b Plate 3-1c Plate 3-1d Plate 3-1e Plate 3-1f Plate 3-1g Plate 3-1h Plate 3-1i Plate 3-1j Plate 3-1a Return to text. Return to image plate. Plate 3-1b Return to text. Return to image plate. Plate 3-1c Return to text. Return to image plate. Plate 3-1d Return to text. Return to image plate. Plate 3-1e Return to text. Return to image plate. Plate 3-1f Return to text. Return to image plate. Plate 3-1g Return to text. Return to image plate. Plate 3-1h Return to text. Return to image plate. Plate 3-1i Return to text. Return to image plate. Plate 3-1j Return to text. Return to image plate. Leukocytosis Diagnostic Significance: Leukocytosis is defined as the presence of increased leukocyte numbers, which may be caused by an increase in the number of one cell type or a combination of cell types. The significance of a leukocytosis is based on the degree of elevation, the cell types constituting the increase, and the cellular morphology (normal, dysplastic, toxic, neoplastic). Increased numbers of neutrophils secondary to inflammation is the most common cause of a leukocytosis. Plate 3-2 Leukocytosis Next Topic Plate 3-2a Plate 3-2b Plate 3-2c Plate 3-2d Plate 3-2e Plate 3-2f Plate 3-2g Plate 3-2h Plate 3-2i Plate 3-2k Plate 3-2l Plate 3-2m Plate 3-2n Plate 3-2a Return to text. Return to image plate. Plate 3-2b Return to text. Return to image plate. Plate 3-2c Return to text. Return to image plate. Plate 3-2d Return to text. Return to image plate. Plate 3-2e Return to text. Return to image plate. Plate 3-2f Return to text. Return to image plate. Plate 3-2g Return to text. Return to image plate. Plate 3-2h Return to text. Return to image plate. Plate 3-2i Return to text. Return to image plate. Plate 3-2k Return to text. Return to image plate. Plate 3-2l Return to text. Return to image plate. Plate 3-2m Return to text. Return to image plate. Plate 3-2n Return to text. Return to image plate. Leukopenia Diagnostic Significance: Leukopenia is defined as a decrease in leukocyte numbers, which is most often caused by a decrease in the number of neutrophils (neutropenia), as neutrophils are the most numerous of the peripheral blood leukocytes. Careful exam of the entire blood smear is emphasized by the fact that sometimes during blood smear preparation, the leukocytes can be concentrated on the feathered edge. In this case, the monolayer will contain very few leukocytes, suggesting an artifactual leukopenia if the monolayer only, and not the entire slide, is examined for WBC estimation. Plate 3-3 Leukopenia Artifactual leukopenia. A, Monolayer, devoid of leukocytes B, Same smear where leukocytes are concentrated on the feathered edge Next Topic Plate 3-3a Plate 3-3b Plate 3-3c Plate 3-3d Plate 3-3e Plate 3-3f Plate 3-3g Plate 3-3h Plate 3-3i Plate 3-3j Plate 3-3a Return to text. Return to image plate. Plate 3-3b Return to text. Return to image plate. Plate 3-3c Return to text. Return to image plate. Plate 3-3d Return to text. Return to image plate. Plate 3-3e Return to text. Return to image plate. Plate 3-3f Return to text. Return to image plate. Plate 3-3g Return to text. Return to image plate. Plate 3-3h Return to text. Return to image plate. Plate 3-3i Return to text. Return to image plate. Plate 3-3j Return to text. Return to image plate. Return to text. Return to image plate. Neutrophils Neutrophils are the most abundant of the granulocytic cell types. Maturation stages from least mature to most mature are: myeloblasts, promyelocytes, myelocytes, metamyelocytes, band neutrophils, and mature (segmented) neutrophils. As cells mature, they decrease in size, the cytoplasm becomes less blue and eventually becomes clear to lightly colored, and the nucleus becomes more condensed and eventually lobulated. Neutrophils are released from bone marrow into circulation in an age-related fashion, with the most mature cells (mature neutrophils) released first. The bone marrow has a storage pool of mature neutrophils, so immature forms are not released into the circulation until the demand (severe, acute infection and inflammation) for neutrophils exceeds the storage pool’s ability to supply adequate numbers of mature cells. Increased numbers of immature neutrophils in the peripheral blood is referred to as a “left shift” and is the hallmark of acute inflammation. Immature neutrophils are also released in an age-related fashion, and as such, the immature neutrophil stage primarily seen in peripheral blood during a left shift is the band neutrophil, with less mature stages seen only rarely. In general, the more severe the systemic inflammation, the higher the number of neutrophils with increased numbers of immature forms present. The morphology and diagnostic significance of the various neutrophil maturational stages and the abnormalities that occur in the neutrophil series are discussed below. Mature (Segmented) Neutrophils Distinctive Features: Mature neutrophils of dogs and cats have similar morphologies. Neutrophils are round and approximately 10 to 12 micrometers (µm) in diameter. The cytoplasm is clear, moderately abundant, and may contain a few very indistinct, faint pink granules, and/or small clear vacuoles, or both. The nucleus is highly condensed and lobulated, generally containing three or four lobules. Nuclear lobes may be connected by a thin strand of chromatin, but more commonly, simply a narrowing of the chromatin exists between lobes to about one third the diameter of the thick portion of the lobules. Diagnostic Significance: Mature neutrophil numbers are increased (neutrophilia) in conditions such as epinephrine release (from excitement), endogenous steroids (stress resulting in glucocorticoid release), steroid administration, inflammation (infectious and noninfectious causes), tissue necrosis, and neoplasia. Mature neutrophilia caused by inflammation is often associated with an increase in band neutrophils (left shift). Leukemoid response is a term used to describe a marked neutrophilia, often with a left shift, which may be seen with severe, acute, focal inflammation (i.e., pyometra, peritonitis, pyothorax, severe abscessation). A persistently increasing, moderate to marked neutrophilia, in which a source of inflammation, infection, tissue destruction, or necrosis cannot be found, should raise the suspicion for chronic granulocytic leukemia. Mature neutrophil numbers are decreased (neutropenia) by conditions such as overwhelming bacterial infections, viral infections (parvovirus, panleukopenia, feline leukemia virus [FeLV]), certain bacterial infections (Salmonella), rickettsial infections (i.e., chronic ehrlichiosis), endotoxemia (infection with gram-negative bacteria), chemotherapeutic agents, bone marrow necrosis, myelophthesic diseases (bone marrow infiltration with neoplastic cells), and bone marrow suppression or failure (i.e., drug-induced neutropenia, immune-mediated neutropenia, cyclic hematopoiesis). Plate 3-4 Normal Mature Segmented Neutrophils Next Topic Plate 3-4a Plate 3-4b Plate 3-4c Plate 3-4d Plate 3-4e Plate 3-4f Plate 3-4g Plate 3-4h Plate 3-4i Plate 3-4j Plate 3-4a Return to text. Return to image plate. Plate 3-4b Return to text. Return to image plate. Plate 3-4c Return to text. Return to image plate. Plate 3-4d Return to text. Return to image plate. Plate 3-4e Return to text. Return to image plate. Plate 3-4f Return to text. Return to image plate. Plate 3-4g Return to text. Return to image plate. Plate 3-4h Return to text. Return to image plate. Plate 3-4i Return to text. Return to image plate. Plate 3-4j Return to text. Return to image plate. Band Neutrophils Distinctive Features: Band neutrophils are similar in size and appearance to mature neutrophils except that the nuclei are nonsegmented (band shaped) or only slightly constricted, and nuclear chromatin is not as tightly clumped. The classic band neutrophil has a plump C-shaped or S-shaped nucleus, with parallel sides, a smooth nuclear margin, and a fairly constant width. If slight constricted areas are present, they are more than one third the width of the rest of the nucleus, distinguishing the bands from mature neutrophils, which have constricted areas of less than one third the width of other areas of the nucleus. The nuclear chromatin is less dense than that of a mature neutrophil. The cytoplasm remains clear unless toxic change is present. Diagnostic Significance: Band neutrophils are either absent or present in very low numbers in healthy dogs and cats. A left shift is the hallmark of acute inflammation. Systemic inflammatory mediators travel to bone marrow, resulting in the production and release of neutrophils. Despite this systemic response, the inflammation may be focal (i.e., pyometra) or diffuse (i.e., bacterial sepsis). Additionally, not all focal areas of inflammation induce a systemic response. For example, cystitis (inflammation of the bladder) is not generally associated with an increased number of band neutrophils. Chronic granulocytic leukemia may also cause an increase in band neutrophil numbers. Also, pseudo–band neutrophils (hyposegmented mature neutrophils) may be seen in Pelger-Huët anomaly (discussed later). A left shift may be regenerative or degenerative. A regenerative left shift is a predominance of mature neutrophils (neutrophilia) with fewer bands, indicating a normal response to inflammation. A degenerative left shift occurs when bands (and often more immature forms of neutrophils) exceed the number of mature neutrophils. Often, a concurrent neutropenia exists. This indicates neutrophil production is not able to meet demand and is associated with a guarded or poor prognosis. Toxic changes are frequent with degenerative left shifts. As band neutrophils are the most common immature neutrophil released into peripheral blood and cannot be distinguished from mature neutrophils with current hematology analyzers, blood smear evaluation is extremely important in identifying and quantitating a left shift. Plate 3-5 Band Neutrophils A, Band neutrophils. Note the open chromatin B, Neutrophils with Pelger-Huët Anomaly. Note the condensed chromatin Next Topic Plate 3-5a Plate 3-5b Plate 3-5c Plate 3-5d Plate 3-5e Plate 3-5f Plate 3-5g Plate 3-5h Plate 3-5i Plate 3-5j Plate 3-5a Return to text. Return to image plate. Plate 3-5b Return to text. Return to image plate. Plate 3-5c Return to text. Return to image plate. Plate 3-5d Return to text. Return to image plate. Plate 3-5e Return to text. Return to image plate. Plate 3-5f Return to text. Return to image plate. Plate 3-5g Return to text. Return to image plate. Plate 3-5h Return to text. Return to image plate. Plate 3-5i Return to text. Return to image plate. Plate 3-5j Return to text. Return to image plate. Return to text. Return to image plate. Metamyelocytes Distinctive Features: Metamyelocytes are about the same size to slightly larger than mature and band neutrophils. The nuclei have one margin indented more than 25% into the nucleus and have an indented or kidney-shaped nucleus. The nuclear chromatin is readily recognized as condensed but generally less so than that of band neutrophils. The cytoplasm is nearly colorless but more basophilic than the nontoxic band neutrophil. Diagnostic Significance: Metamyelocytes are rarely seen in the peripheral blood of healthy dogs and cats. Metamyelocytes are sometimes seen in peripheral blood during severe inflammation along with band neutrophils as part of a left shift. Granulocytic leukemia may also cause an increase in metamyelocytes but occurs rarely. Also, pseudometamyelocytes (hyposegmented mature neutrophils) may be seen in Pelger-Huët anomaly (discussed later). Plate 3-6 Metamyelocytes Next Topic Plate 3-6a Plate 3-6b Plate 3-6c Plate 3-6d Plate 3-6e Plate 3-6f Plate 3-6g Plate 3-6h Plate 3-6i Plate 3-6j Plate 3-6a Return to text. Return to image plate. Plate 3-6b Return to text. Return to image plate. Plate 3-6c Return to text. Return to image plate. Plate 3-6d Return to text. Return to image plate. Plate 3-6e Return to text. Return to image plate. Plate 3-6f Return to text. Return to image plate. Plate 3-6g Return to text. Return to image plate. Plate 3-6h Return to text. Return to image plate. Plate 3-6i Return to text. Return to image plate.< div class='tao-gold-member'> Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Related Related posts: 6: Extracellular Organisms 4: Platelets 1: General Assessment 5: Hematopoietic Neoplasia Stay updated, free articles. Join our Telegram channel Join Tags: Atlas of Canine and Feline Peripheral Blood Smears Jul 24, 2016 | Posted by admin in SMALL ANIMAL | Comments Off on 3: White Blood Cells Full access? Get Clinical Tree