CHAPTER 15. Surgery of the Mare Reproductive Tract
OBJECTIVES
While studying the information covered in this chapter, the reader should attempt to:
■ Acquire a working knowledge of the conformational defects acquired through injury during parturition or that develop insidiously in aged, multiparous mares.
■ Acquire a working understanding of the surgical procedures and techniques used to correct conformational abnormalities that contribute to infertility in the mare.
STUDY QUESTIONS
1. Discuss injuries that occur during parturition and result in abnormal conformation of the genital tract.
2. Discuss conformational defects of the urogenital tract that occur in aged, multiparous mares and contribute to infertility.
3. Describe procedures and techniques for a Caslick’s vulvoplasty.
4. Describe the procedure for a breeding stitch in the vulva.
5. Describe the procedure for a perineoplasty (i.e., vestibuloplasty).
6. Describe the procedure used to create a urethral extension for treatment for urine pooling.
7. Describe the procedure used to treat a mare with a third-degree perineal laceration.
8. Describe the procedure used to treat a mare with a rectovaginal fistula.
9. Describe the procedure for treating a mare with a cervical laceration.
10. List preoperative and postoperative considerations for urogenital surgery in the mare.
Surgical procedures performed on the mare reproductive tract (with the exceptions of cesarean section, surgical correction of uterine torsion, and ovariectomy) are performed primarily to correct urogenital abnormalities that contribute to contamination of the reproductive tract. Contamination results from injuries that occur during parturition or from conformational changes that occur as mares age. This chapter discusses only the most common surgical procedures performed to reconstruct vulvar, vestibular, and cervical abnormalities. For more detailed descriptions of these and other surgical procedures involving the reproductive tract, the reader should refer to veterinary medical-surgical texts.
SELECTION OF CANDIDATES FOR SURGERY
Mares with conformational changes of the urogenital tract that can be corrected with surgical reconstruction are candidates for surgery, provided that the results of a thorough breeding soundness examination indicate that the procedure has a good chance of restoring the mare’s fertility. An exception to the need for a breeding soundness examination is a mare with a rectovestibular laceration or fistula, because these injuries nearly always arise in fertile, young mares during foaling as a result either of fetal malposture during delivery or inadequate dilation of the caudal birth canal sufficient to allow foal passage without tissue disruption. Indeed, such a mare has no reason to be infertile once contamination of the reproductive tract is prevented by surgical reconstruction. However, for other procedures used for surgical correction of reproductive abnormalities, a breeding soundness examination is indicated to assess the breeding potential of the mare. If severe and irreparable damage to the endometrium, cervix, vagina, or vestibule has occurred, the owner may elect not to invest time and money into surgery and aftercare.
Before any surgical procedure is performed, the practitioner should ensure that the mare has been adequately immunized against tetanus.
Defects commonly corrected with reconstructive surgery of the reproductive tract include the following:
■ Pneumovagina caused by a cranially sunken anus and tipping of the vulva (see Figure 1-12).
■ Urovagina caused by cranioventral deviation of the vagina, which pulls the urethral orifice cranially, resulting in urine splashing into the vestibule and vagina during urination (see Figure 4-19).
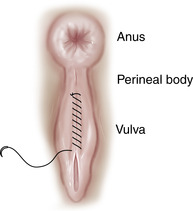
Perineal injuries occur during foaling and are characterized by tearing of the shelf between the rectum and vestibule (Figure 15-1). Third-degree perineal lacerations or rectovestibular lacerations (the most severe type of perineal injury) are those that extend from the vestibule into the lumen of the rectum and through the perineal body. A laceration through the dorsal aspect of the vestibule that perforates the rectum but does not disrupt the perineal body is termed a rectovestibular fistula. The fistula often results in contamination of the vestibule and vagina with feces, but because the perineal body is intact, the laceration may not be readily apparent (Figure 15-2). Cervical lacerations arise from tearing of an insufficiently dilated cervix during normal delivery or during dystocia (see Figure 4-12).


PNEUMOVAGINA
Pneumovagina is a condition leading to constant fecal contamination of the vestibule and vagina because of conformational faults that cause a mare to aspirate air into the tubular portion of the reproductive tract. The condition is commonly called “wind sucking” and usually culminates in ascending infection of the vagina, cervix, and endometrium. Causes of pneumovagina include tearing or stretching of the vulvar seal or the vulvovaginal sphincter (see Chapter 1) and a sunken perineal body, characterized by cranial displacement of the anus and resulting in tipping of the vulva cranially over the brim of the pelvis (see Figure 1-12). The condition is quite common in underweight, aged, pluriparous mares.
The most common surgical procedure used to correct pneumovagina is the Caslick’s operation, sometimes referred to as a vulvoplasty. For a Caslick’s vulvoplasty, the mare is placed in a stock, and her tail is wrapped and directed away from the perineum. The perineum and vulva are scrubbed with a disinfectant soap, rinsed, and dried, and the dorsal aspect of the mucocutaneous margin of each labium is desensitized with a local anesthetic solution, such as lidocaine. The mare can be sedated, or a twitch can be applied to its upper lip to prevent the mare from moving excessively during infiltration of the labia with local anesthetic solution. The local anesthetic solution is injected subcutaneously at the dorsal commissure of the vulva (Figure 15-3) and infiltrated along the margin of each labium to slightly below the floor of the ischium. The level to which the margins of the labia are sutured ventrally can be determined by placing firm pressure with the fingers on either side of the vulva and pressing down to locate the ischium. If the labia are not sutured to slightly below the floor of the ischium, the vulva may migrate far enough cranially, as the mare moves, to permit air to be aspirated into the vagina. Care should be taken to ensure that the ventral portion of the vulva remains spacious enough to allow urine to escape during urination, insertion of the stallion’s penis during copulation, and insertion of a vaginal speculum, if the mare is to be bred via artificial insemination. If the ventral aspect of the vulva is sufficiently spacious, the surgeon should be able to easily insert four fingers into the vulvar opening after the operation is completed.

After the mucocutaneous margin of the right and left labia is infiltrated with local anesthetic solution, a thin strip of tissue, approximately 0.5 cm wide, is removed at the mucocutaneous junction of each labium with scissors (Figure 15-4). Removal of strips wider than this results in a large scar, which complicates subsequent Caslick’s operations. The margins of the labia are apposed intimately with no. 0 or 00, nonabsorbable sutures (Figure 15-5). The type of suture pattern used is not important, if the labial margins are closely apposed, because little tension is exerted on the suture line. Patterns commonly used include simple continuous, continuous interlocking, and continuous horizontal mattress. Sutures should be removed at 10 to 14 days, at which time the wound should be healed.

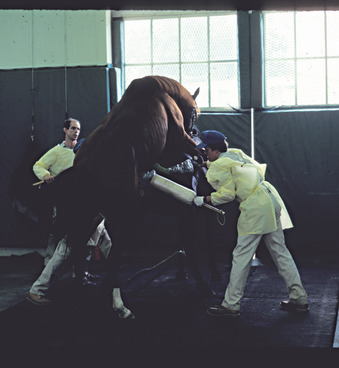
If the labia must be opened for breeding, for vaginal examination, or for unobstructed foaling, they should be reapposed when a large vulvar opening is no longer necessary. A breeding stitch is a single, simple interrupted suture sometimes placed at the ventral aspect of the vulvar closure to preclude the need to open the sutured labia of a mare that must be bred (Figure 15-6). Umbilical tape or heavy, polymerized caprolactam suture (e.g., Vetafil, S. Jackson Co, Washington, D.C.) is commonly used for the breeding stitch. The suture bite should extend at least 1 cm abaxial to the margin of each labium, and the deep portion of the suture should be buried in the labial submucosa so that it does not abrade the stallion’s penis during breeding. The suture is placed loosely enough to allow stretching of the ventral aspect of the sutured labia, but not so loosely that it allows the sutured tissue to tear. Use of a breeding roll helps to limit the extent of penile intromission during natural service to avoid tearing of the sutured tissue or the breeding stitch (Figure 15-7).

The entire vulva of a mare with an extremely sunken anus and perineal body may be deviated so far cranially and ventrally that the vulvar cleft assumes a nearly horizontal position over the ischium. A Caslick’s suture may not correct pneumovagina in such mares or may prevent the mare from adequately expelling urine. For prevention of both pneumovagina and urine pooling caused by this extreme conformational abnormality, the perineal body must be reconstructed (i.e., perineoplasty or vestibuloplasty). We often perform a modified vestibuloplasty, as described by Slusher (1986). This vestibuloplasty entails removal of an isosceles triangle of mucosa from the dorsal aspect of the vestibule.
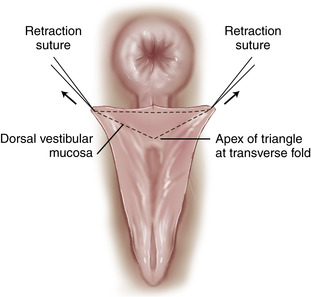
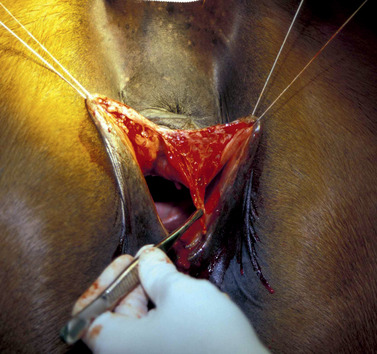
In preparation for reconstruction of the perineal body, as described by Slusher (1986), the mare is sedated, and the perineum is desensitized with administration of 2% lidocaine or mepivacaine (1 to 1.25 mL/100 kg) through an 18- or 20-gauge, 1.5-inch (3.8-cm) needle inserted into the epidural space. The dorsal aspect of the vestibule is exposed by retracting each labium laterally, with a loose suture or Backhaus towel clamp placed through the labium at the juncture of its dorsal one third and ventral two thirds and with retraction of the dorsal commissure of the vulva dorsally and caudally, also with a loose suture or towel clamp (Figure 15-8). A point on the dorsal aspect of the vestibule that lies directly beneath the anus is marked to serve as the apex of a triangle of mucosa to be removed. The distance between this mark and the dorsal commissure of the vulva is measured, and one half of this distance from the dorsal commissure of the vulva is marked on the mucocutaneous margin of each labium. A line between these two points on the labia serves as the base of the mucosal triangle to be removed (Figure 15-9).

 |
| Figure 15-9 |
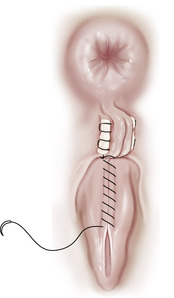
The points of the triangle are connected with a scalpel, and the mucosa overlying this area is removed (Figure 15-10). Two or three, no. 1 or 2 nonabsorbable sutures are placed horizontally through the perineum in a line from the apex of the triangle to the base, as shown in Figure 15-11. Small rolls of gauze swabs work well as stents to prevent the sutures from pulling through the skin. Just enough tension is placed on the sutures to bring the triangular area into a vertical position. Sutures are removed in 5 to 10 days. Excessive tension placed on the sutures can cause tissue necrosis. If sutures begin to cause tissue necrosis, they can be removed, one daily or at alternate-day intervals, to relieve pressure. This surgical procedure effectively increases the area of the perineal body and returns the vulva to a more vertical position (Figure 15-12), but the sunken position of the anus remains unchanged. If the procedure is done properly, the vulvar opening is not diminished appreciably, and the mare can be bred with natural service.
 |
| Figure 15-10 |
 |
| Figure 15-11 Modified perineoplasty. Two or three retention sutures are placed horizontally in a line from the apex to the base of the triangle shown in Figure 15-10. Small rolls of gauze or rubber tubing can be placed in the loops of the retention sutures to distribute pressure and avoid pressure necrosis. |
 Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|