CHAPTER 22 Ultrasonography of the Young Patient
Equipment
Pediatric dogs and cats are best evaluated using an ultrasound machine equipped with a curvilinear, phased array, blended frequency scanhead (Figure 22-1, A). However, an ultrasound machine with a curvilinear variable frequency scanhead (5.0 to 8.0 MHz) is also satisfactory. Many portable machines now have a high frequency linear scanhead (8.0 to 10.0 MHz) available, which improves image quality and also allows evaluation of smaller, superficial regional anatomy (e.g., thyroid, parathyroid, and cryptorchid testes) (Figure 22-1, B).


Preparation
The pediatric patient can be placed in dorsal or lateral recumbency for the study. The authors prefer dorsal recumbency within a padded V-trough, which allows less clipping of the haircoat and permits a clockwise scan of the viscera (see below). Optimally, the pediatric dog or cat is gently restrained by assistant(s) holding the forelimbs and hindlimbs (Figure 22-2). Sedation is rarely required for the basic abdominal scan unless marked pain or apprehension is present. By allowing the patient to become accustomed to this positioning before initiating clipping or scanning, struggling and resultant aerophagia are minimized.

The Normal Abdomen
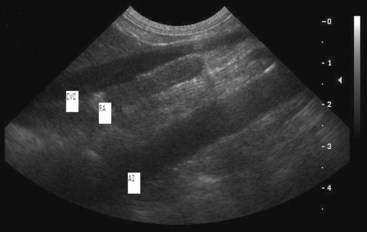
Regardless of the clinical history, the abdomen should be evaluated methodically. With the animal in dorsal recumbency, place the scanhead under the xyphoid with the beam in the sagittal plane (Figure 22-3). Visualization of the liver is best achieved by adjusting the depth of the image to include the hyperechoic arc of the diaphragm. Then, in the sagittal plane, pointing the beam toward the patient’s right elbow allows visualization of the gall bladder. Fanning the beam from the right to the left elbow maximizes visualization of the liver in the sagittal plane. The gall bladder is seen on the right; the left liver lobes are seen ventral to the stomach. The ultrasonographic appearance of the normal hepatic parenchyma permits differentiation of portal and hepatic vessels. The gall bladder should be thin walled and the fluid within very anechoic. Size can be variable and is usually not correlated with clinical disease in the young animal. The normal-sized liver does not extend caudally beyond the stomach. Turning the beam to transverse allows for visualization of the liver between the gall bladder and stomach. This view is good for evaluation of the hepatic border at its interface with the falciform fat in the near field, echogenicity of hepatic parenchyma, and portal architecture. The portal vessels have very echogenic walls compared with the hepatic veins (Figure 22-4).


Figure 22-4 Portal veins have hyperechoic wall; hepatic vessels do not. PV, Portal vein; HV, hepatic vein.
After completing evaluation of the liver, resume the sagittal plane; scan clockwise to the upper left quadrant of the patient past the stomach to the spleen. The spleen will be visualized ventrally along the left body wall in the near field. Splenic border, parenchyma, echogenicity, and shape should be evaluated. Splenic parenchyma should be more echogenic and have a more homogeneous echotexture than liver. A transverse image of the spleen can be obtained by scanning to the caudal edge of the left rib cage and pointing cranially in cross-section. This transverse view evaluates the spleen as it follows the left body wall (Figure 22-5).

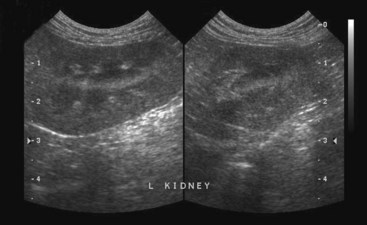
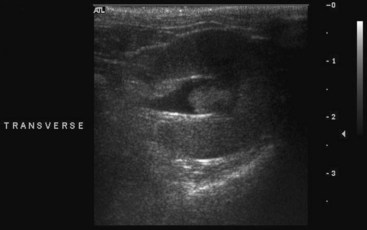
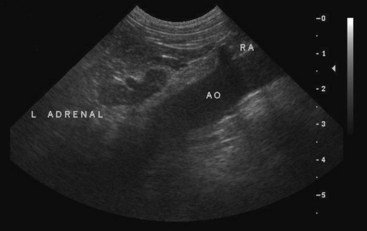
Following the spleen transversely down the left body wall, you will see the left kidney. Once visualization of the kidney is achieved, turn to the sagittal plane and produce a long axis view of the left kidney. Now evaluate the renal border, cortex echogenicity, corticomedullary interface, and pelvic architecture (Figure 22-6). Dilation of the renal pelvis should be evaluated and confirmed in both scan planes. The transverse image is best for confirmation of renal pelvic dilation (Figure 22-7). The left adrenal gland is located medial to the left kidney anywhere along its length. Isolation of the left adrenal gland is best achieved by locating the linear aorta and the branching arteries (celiac, cranial mesenteric, and renal). In the sagittal plane, with strong hand pressure, sweep medially from the left kidney to find the aorta. Now find the branching renal artery. The left adrenal gland is located cranial to the left renal artery and caudal to the left cranial mesenteric artery. The left adrenal gland is visualized as a bilobed structure with the phrenicoabdominal vein at its waist (Figure 22-8). This completes evaluation of the upper left abdominal quadrant.
Now with a transverse beam placed perpendicularly in the middle of the abdomen, scan caudally to a large hypoechoic structure, the urinary bladder. Evaluate the ventral bladder wall and urinary bladder lumen contents, and then the dorsal bladder wall. The normal bladder wall is uniform in thickness, and the contents are anechoic. The major vessels (caudal vena cava and aorta) will be located dorsal to the bladder, seen as two large black discs. Sublumbar lymph nodes can be seen at the aortic bifurcation into the iliac arteries, adjacent to the dorsal urinary bladder wall (Figure 22-9, A). Sagittal scanning of the urinary bladder caudally allows visualization of the urethra (and prostate in the male) (Figure 22-9, B).

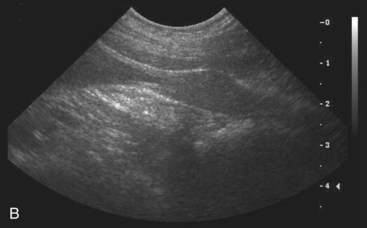
Figure 22-9 A, Transverse urinary bladder with major vessels and sublumbar node. B, Normal puppy prostate.
Evaluation of the upper right abdominal quadrant should include the right kidney, right adrenal, duodenum, and right limb of the pancreas. The right kidney is found at the edge of the right rib cage in the renal fossa of the liver. Obtain images of the right kidney in the sagittal and transverse scan planes. The right kidney should be evaluated as was the left kidney (i.e., renal border, cortical echogenicity, corticomedullary interface, and pelvic architecture). By scanning sagitally between the right kidney and the caudal vena cava with a fanning technique, as well as the scanhead pointed slightly cranially, the major vessels (vena cava and aorta) will be visualized as two hypoechoic ribbons running across the image from the 8 o’clock position to the 2 o’clock position. The right adrenal gland can be located, visualized, and evaluated for size and shape just lateral to the caudal vena cava (Figure 22-10).
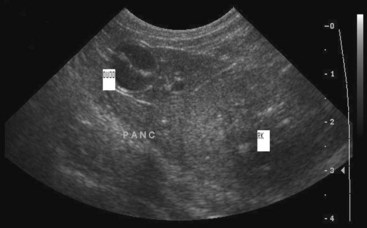
In the transverse plane, return to the right kidney and lateral to the kidney, the duodenum. In the dog, at the cranial pole of the kidney adjacent to the duodenum will be the right limb of the pancreas. The right pancreatic limb border may not be seen but is identified by visualizing the caudal pancreaticoduodenal vein (Figure 22-11). Turning to the sagittal plane, follow the pancreas, scanning medially to the angle of the body and left limb. The pancreatic body is seen caudal to the stomach and cranial to the splenic vein. The left limb of the pancreas is found caudal to the splenic vein and midline to the cranial pole of the left kidney (Figure 22-12). In the cat, in the sagittal plane, the right limb of the pancreas is identified just caudal to the duodenum, which is itself caudal to the gall bladder. Localizing the feline right pancreatic limb varies because the feline duodenum is situated more medially with more cranial flexure than in the canine (Figure 22-13). The normal pancreas is usually not well visualized because its acoustic impedance is similar to the surrounding mesentery.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


