CHAPTER 36Trauma to the Penis
Traumatic injury of the penis in horses is not common.1,2 Kick-related injury to the penis and prepuce of stallions and aggressive geldings by seasonal mares is likely the most frequent origin of trauma to this region.1,2 Horses can also experience blunt trauma from obstacles or objects either in competitive pursuits or during playful activity. Lacerations and penetrating injury can also occur from a variety of sources.
TRAUMA WITHOUT OPEN WOUNDS
Blunt trauma to the penis/prepuce is likely the most common reason a veterinarian is asked to examine this region in an adult male horse. A complete physical examination should be performed with obvious attention to the external genitalia. Swelling that is marked in the acute phases after injury should be closely evaluated for the presence of a hematoma in which the hemorrhage is ongoing. The best detection method for this instance is likely ultrasonography.3 It is not recommended to perform needle aspirates at this time due to the possibility of inoculating microorganisms into a potentially sterile site. Ultrasonography may also assist in the evaluation of established swelling because edema fluid will typically have a more echo-dense appearance than free fluid/blood.3
Acute hematoma formation should be treated as for any other episode of substantial hemorrhage.1,2,4 Local tissue cooling with ice packs, cold running water, and local tissue pressure should be initiated at the earliest possible opportunity. The penis and prepuce should be compressed and elevated with a bandage or sling to approximate these tissues to the ventral body wall. If swelling is confined to the glans, a circumferential pressure bandage can assist in the reduction and resolution of bleeding and swelling. This should be maintained at all times other than when local, topical treatment is applied. The application of topical ointments, salves, and astringent agents should be approached carefully so that the skin is not irritated, which can exacerbate local swelling. Emollient ointments can assist some horses. Preparations with dimethyl sulfoxide (DMSO), lanolin, Furacin, petroleum jelly, and formulas for topical udder treatment in cattle can help keep penile and preputial skin protected from desiccation when retraction to normal position is not possible.1
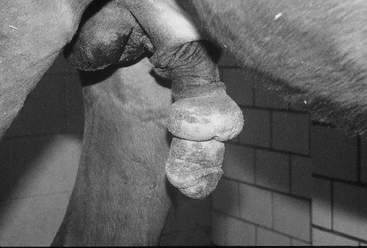
Blunt trauma can result in permanent penile dysfunction. Paraphimosis and priapism can both result from trauma to the penis and prepuce (Figure 36-1). Repositioning of the penis into the prepuce and return to normal function are the obvious goals of treatment for these disorders.1,5–7
If manual replacement of the penis into the sheath can be accomplished with little difficulty, a purse-string suture at the preputial orifice may successfully restrain the penis until swelling is resolved and function returned. This appears to be rarely successful, however. An alternative treatment for paraphimosis is the retraction and retention of the penis within the prepuce via a sutured, phallopexy procedure, the Bolz technique.1,2 The retracted penis is fixed into position within the external lamina of the prepuce by making a longitudinal incision 10 cm caudal to the scrotum over the perineal raphae. The penis is dissected free of surrounding fascia and is retracted into the prepuce. This will create a sigmoid flexure to the penis, but this has not been associated with complications. The penis is secured into position with large (No. 2) nonabsorbable sutures or umbilical tape through the annular ring of the penis, which exit the skin 2 cm apart and 4 cm from the edge of the incision. The suture can be tied at the skin or secured over roll gauze. The penis should be retracted such that the rostral end of the glans is aligned with the preputial orifice. Sutures can be removed at 2 weeks after placement. If this technique fails to result in permanent return to normal penile position, more aggressive surgical treatment may be required.1,2
Occasionally horses with paraphimosis can be successfully managed with surgical treatment.1,6
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


