Chapter 76 Thiafentanil Oxalate (A3080) in Nondomestic Ungulate Species
Features of Thiafentanil Oxalate
Clinical Considerations
The advantage of thiafentanil oxalate compared with the previously mentioned opioids (etorphine and carfentanil) is a shortened induction time, by as much as 50%, while still retaining equivalent agonist activity.7 In an elk study, thiafentanil oxalate was found to have 63% the potency; in another study, it was found to have higher potency than carfentanil HCl and twice the potency of etorphine.18,23,24 In cervids, the induction time was found to be shortened by 26% to 65% when compared with carfentanil. Thiafentanil appears to be not only more rapidly absorbed, but also more rapidly metabolized in those species in which it has been tested in. In ferrets, recovery from thiafentanil oxalate anesthesia was found to be two to four times more rapid when compared with carfentanil. Because of the shortened half-life, opioid renarcotization has not been a problem. This is a particularly important feature when working with free-ranging wildlife. Renarcotization is dangerous for free-ranging wildlife because prolonged struggling during recovery may lead to several life-threatening sequelae, such as hyperthermia, trauma, capture myopathy, and predation. There are multiple reports of complete thiafentanil oxalate reversal with the antagonist naltrexone, with no renarcotization.* Elk immobilized with thiafentanil oxalate and not reversed with an antagonist recovered spontaneously in 27 to 106 minutes, depending on the initial dose of thiafentanil oxalate. If the targeted free-ranging nondomestic ungulate escapes capture when darted, it may still successfully recover without the administration of an antagonist.
Thiafentanil oxalate is currently approved and registered for use in the Republic of South Africa. There is now a wealth of knowledge and experience with its use in African species. Published reports date back to a 1993 peer-reviewed study performed in Kruger National Park, South Africa.12 Several current veterinary textbooks on exotic and wildlife capture recommend thiafentanil oxalate as a drug of choice.8,26 A veterinary textbook on the subject of African wildlife anesthesia contains many protocols for the administration of thiafentanil oxalate to African ungulate species.13 In North America, there have been several peer-reviewed articles on its use in North American ungulate species.* It has become the drug of choice for the American pronghorn antelope.16 One of the authors (DK) has successful experienced using thiafentanil oxalate in several captive and free-ranging African, North American, and Asian nondomestic ungulate species.3 Finally, perhaps the most popular veterinary textbook on wildlife and zoologic immobilization describes thiafentanil oxalate immobilization protocols for several North American ungulate species and many African species.15 As is the case with carfentanil, thiafentanil oxalate does not seem to be effective in nondomestic ungulates in the family Equidae.20 Specific mention was made of Burchell’s zebra (Equus burchellii). Thiafentanil oxalate plus a sedative was moderately effective with captive Grevy zebra (Equus grevyi) and Przewalski’s horse (Equus prezewalskii) in a North American zoological institution but not equal to etorphine. If etorphine is available, it continues to be the drug of choice for Equidae.
As with other opioids, all species may show signs of excitement, tachycardia or tachypnea, bradycardia or bradypnea, hypertension or hypotension, depressed respiration, cyanosis, poikilothermia, and reaction to sudden noise when immobilized with thiafentanil oxalate. In elk, only high doses of thiafentanil oxalate (10 µg/kg body weight [BW]) have an effect on respiratory rate; very high doses (50 µg/kg BW) cause only modest decreases in respiratory rate and no significant decreases in heart rate.25 Thiafentanil oxalate appears to produce less respiratory and cardiac depression when compared with other potent opioids such as fentanyl, carfentanil, and etorphine.
Thiafentanil oxalate is suitable for use by deep intramuscular injection using remote delivery systems (e.g., pistol, rifle, pole syringe) or by intramuscular or intravenous delivery by a handheld syringe with animals that are manually restrained. Opioid immobilizing agents should never be stored in aluminum darts because potency is lost in a matter of days.14 On occasion, thiafentanil oxalate is used by itself as an immobilizing agent but is more typically combined with tranquilizers (e.g., azaperone), sedatives (e.g., xylazine, medetomidine), and dissociative agents (e.g., ketamine, telazol) as a part of balanced anesthesia protocol. Balanced anesthesia lessens the dose of each agent maximizing their beneficial properties and minimizing the undesirable side effects.
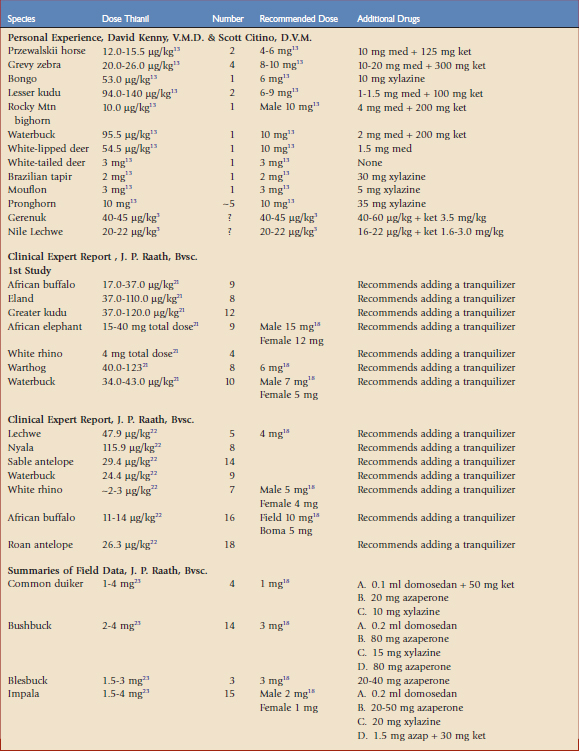
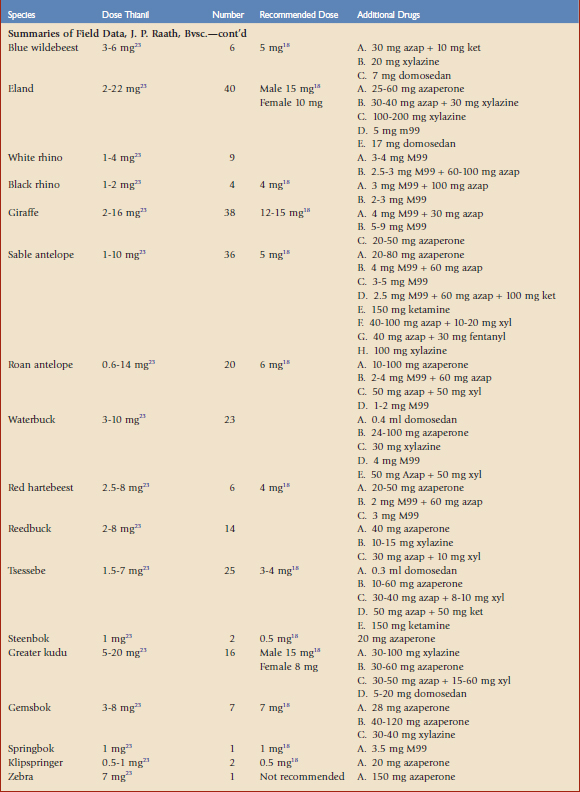
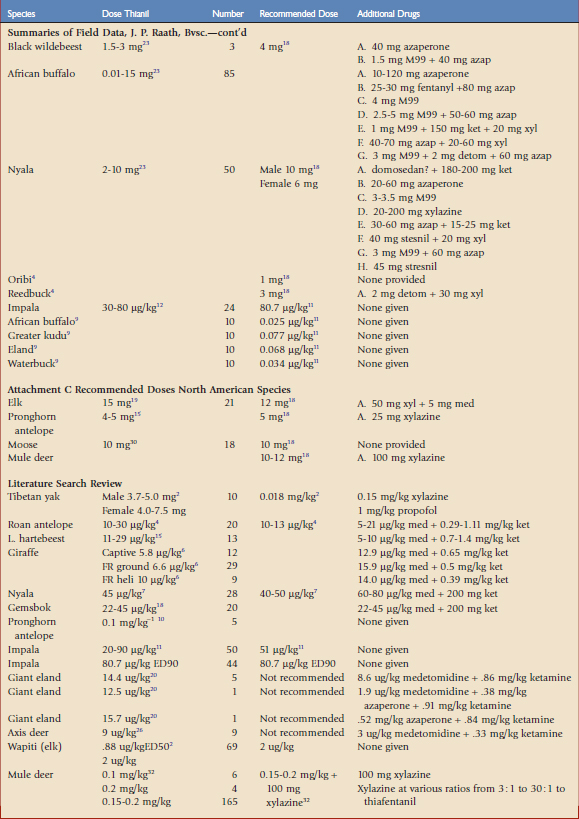
Doses will also vary depending on the situation: captive versus free-ranging animals, agitated versus quiet animals, healthy versus sick animals. In field conditions, it is often desirable to err on the side of overdosing so that the animal does not flee too long and too far, leading to trauma, overheating, and capture myopathy. Specific doses and recommendations are given in Table 76-1 for some nondomestic ungulate species.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


