32 Respiratory emergencies
Feline Pleural Effusion
Theory refresher
Causes
Causes of pleural effusion in cats include:
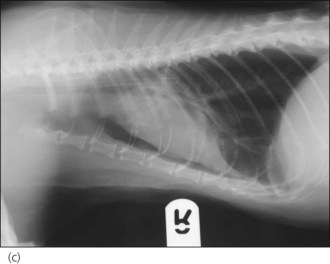
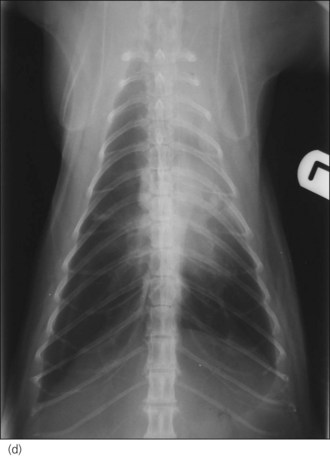
In the author’s experience, neoplasia and congestive heart failure (see Ch. 31) are the two most common causes identified in cats (see Figures 32.1–32.4).

Figure 32.1 Right lateral thoracic radiograph of a cat with pleural effusion secondary to a cranial mediastinal mass.
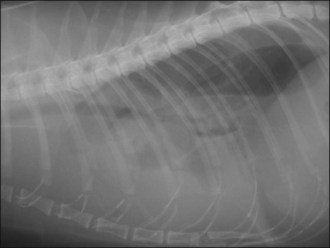
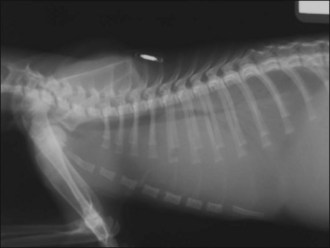
Figure 32.2 Right lateral thoracic radiograph of a cat with severe pleural effusion (diagnosis not made).


Case example 1
Clinical Tip
Further case management
The cat’s respiration had improved to some extent following initial oxygen therapy but there was still a marked increase in respiratory effort. Given the suspicion of pleural effusion, it was decided to perform thoracocentesis for diagnostic and potentially therapeutic purposes (see p. 291). The procedure was only performed on the right side as a large volume of pleural fluid was removed (250 ml, approximately 50 ml/kg) and the cat’s breathing improved significantly almost immediately. The cat was returned to the oxygen cage following thoracocentesis after clipping the fur over both cephalic veins and applying topical local anaesthesia (EMLA® cream 5%, AstraZeneca – see Ch. 5) to both sites. The pleural effusion was grossly milky in appearance. In-house cytology revealed that more than half of the cells present were small lymphocytes, and no bacteria were seen. It was therefore presumptively classified as a chylous effusion but samples had also been collected into additional sterile containers for submission to an external laboratory.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


