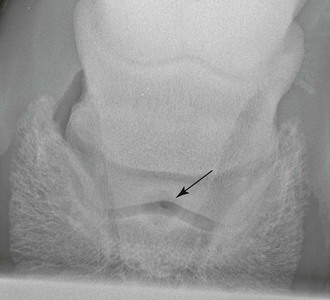
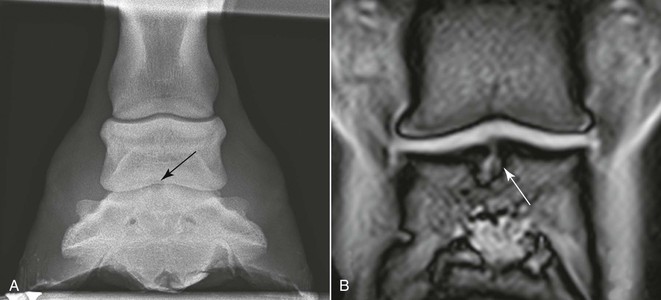
Ceri Sherlock, Tim Mair True bone cysts, defined as a closed cavity lined by epithelium and containing fluid or semi-solid material, are relatively infrequently identified in the horse. Subchondral bone cysts (also called subchondral cystic lesions or osseous cyst–like lesions) are not true bone cysts because they lack an epithelial lining and frequently communicate with an articular surface. These characteristics have resulted in support for the use of the term osseous cyst–like lesions (OCLLs). The phalanges are the second most common anatomic location in which OCLLs are recognized in the horse (26.2% prevalence among all reported OCLLs). Osseous cyst–like lesions are often found on the weight-bearing surface of joints, and most communicate with the joint through tracts of varying sizes. The lesions have marked variation in size (ranging from shallow defects to lesions >10 mm deep) and shape (dome shaped, conical, or spherical). On macroscopic evaluation, OCLLs have a fibrous lining and are filled with fibrous tissue, with or without synovial gelatinous material. Some OCLLs also contain fibrocartilage, which may be partially mineralized, and some may occasionally contain necrotic bone. Fibrous tissue within OCLLs produces nitric oxide, prostaglandin E2, and neutral metalloproteinases. Conditioned media of OCLL tissue harvested arthroscopically induce the recruitment and activation of osteoclasts in vitro. This increased osteoclastic activity is likely to be associated with expansion of cysts in vivo. Osseous sclerosis of varying intensity may surround OCLLs, depending on the stage of development. Osseous cyst–like lesions are generally regarded as multifactorial in etiology. The pathologic processes that have been implicated include genetic causes, growth rate, hormonal and mineral imbalances, osteochondrosis, biomechanics, and trauma. Certain presenting characteristics of the OCLLs may provide an etiologic insight; OCLLs that are bilateral or are found in young horses with no history of trauma are most likely to be developmental, whereas OCLLs detected after a horse has a proven athletic career seem more likely to be traumatic in origin. Developmental diseases such as osteochondrosis arise when endochondral ossification is disturbed. A focal area of retained cartilage may undergo degeneration and subsequently manifest as an OCLL within the bone. Trauma has also been implicated as a potential cause of OCLLs. Osseous cyst–like lesions have been recognized after articular sepsis, osteoarthritis, and intraarticular fractures. Trauma may initiate a cracklike articular cartilage defect that allows pressure from the synovial fluid to cause necrosis and subsequent resorption of the underlying bone, a sequence of events referred to as the hydrostatic theory. It is also possible that trauma causes subchondral bone ischemia and necrosis, followed by revascularization and resorption of necrotic bone, which leaves a subchondral lesion. The role of osseous trauma as a primary cause in the etiology of OCLLs has been supported by observation of lesion formation subsequent to bone marrow lesions (also known as bone bruises, bone edema, bone contusion, and occult fractures). In humans, subchondral cyst–like lesions are also reported as developing subsequent to bone marrow lesions. Physical examination abnormalities in horses with phalangeal OCLLs may be subtle, and specific details are described for each anatomic area below. Lameness in horses with phalangeal OCLLs is variable; some horses develop severe lameness, whereas others have mild intermittent lameness. Some horses have no lameness. The speed of onset of associated lameness is also variable. Lameness may not be appreciated until training is commenced in young horses, whereas there is often a history of previous or ongoing intraarticular inflammation in middle-aged or old horses. Lameness has been attributed to pain originating from the joint (synovitis) or the subchondral bone (increase in intraosseous pressure), an increase in intracystic pressure, or a combination of these. Osseous cyst–like lesions that are close to an articular surface are more likely to be associated with lameness than those that are distant from an articular surface. Lameness can subside with rest but often recurs when exercise resumes. Lameness may be exacerbated by distal limb flexion; however, most horses with phalangeal OCLLs are not responsive to hoof testers. Diagnostic analgesia can be useful to help isolate the location of lameness. Perineural analgesia at the abaxial sesamoid level should alleviate the pain and lameness caused by phalangeal OCLLs. Analgesia of the palmar or plantar digital nerves is inconsistent and often incomplete in lameness resolution, even in horses with distal phalangeal OCLLs. Intraarticular analgesia will often improve the lameness if the OCLL communicates with the joint; however, intraarticular analgesia rarely abolishes the lameness completely. After localization of the lameness, standard radiographic views of the isolated area should be obtained, although OCLLs may not always be identified on such views. The optimal views for identification of OCLLs depend on anatomic location and are described in the following sections. The stage of development influences the ease of identification and radiologic characteristics of OCLLs. Large cysts are relatively easily identified; however, smaller cysts that communicate with the joint can be overlooked. Because there must be a 30% to 50% change in bone density to manifest radiologic change, small, subtle lesions are not easily identified with this modality. Osseous cyst–like lesions may first be identified as a small radiolucent flattening or depression in the articular surface. With progression of pathologic change, a circular, oval, or conical single or multi-chambered radiolucency in the bone may be identified (Figures 191-1 to 191-5). There may be a rim of radiodense sclerosis around the lucency. Thorough examination of the affected joint with specific emphasis on evaluation for degenerative joint disease should be undertaken if an OCLL is detected. Contrast arthrography may be used to evaluate communication between an OCLL and an articular surface.
Phalangeal Subchondral Bone Cysts
Overview of Subchondral Phalangeal Bone Cysts
Terminology and Characterization
Etiology
Investigating the Horse with a Suspected Osseous Cyst–Like Lesion
Physical Examination and Lameness Evaluation
Diagnostic Analgesia
Diagnostic Imaging
< div class='tao-gold-member'>
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Phalangeal Subchondral Bone Cysts
Chapter 191
Only gold members can continue reading. Log In or Register to continue
