Chapter 5 Pathophysiology of heart failure
MECHANISMS OF HEART FAILURE
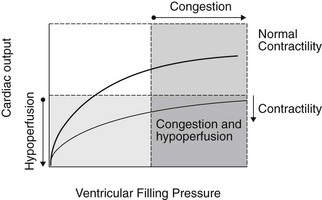
Regardless of the etiology or mechanism of heart failure, CHF is associated with two primary haemodynamic abnormalities: (1) increased ventricular filling pressures and (2) reduced cardiac output. Increased ventricular filling pressures are responsible for signs of congestion and oedema; whereas reduced cardiac output causes clinical signs of inadequate tissue perfusion. The haemodynamic abnormalities and resulting clinical signs that characterize heart failure are illustrated using ventricular function curves in Figure 5.1.
 AF, PC, VMD)
AF, PC, VMD)Only gold members can continue reading. Log In or Register to continue



