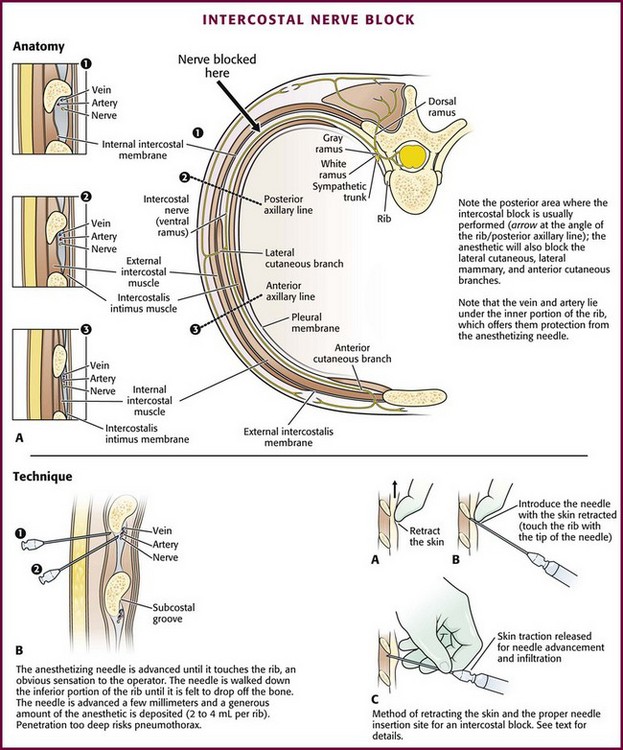
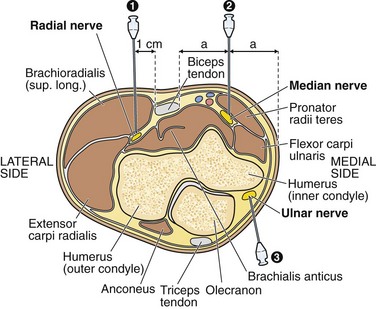
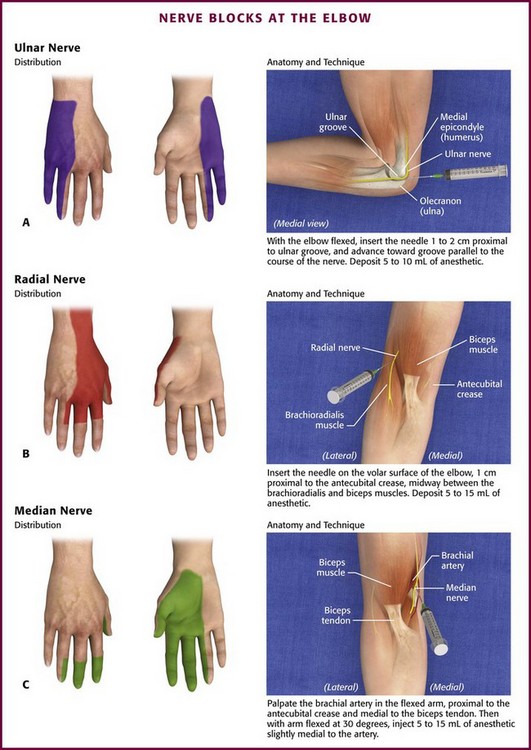
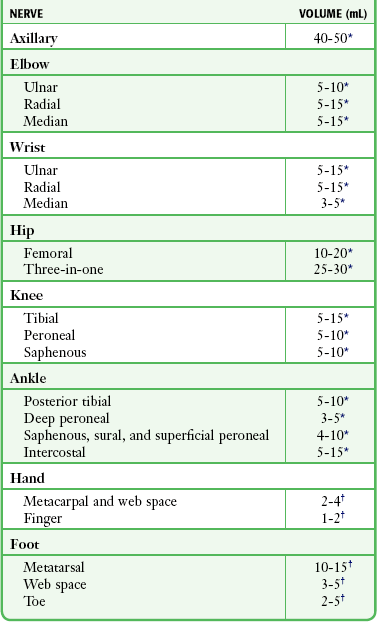
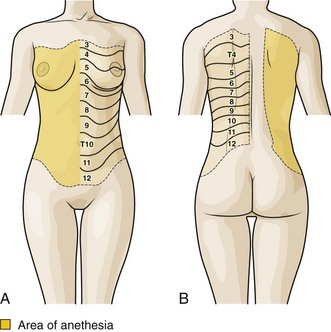
Chapter 31 For most lacerations and injuries seen in the emergency department (ED), local infiltrative anesthesia is adequate and more efficient than using a nerve block (see Chapter 29). Patients who require extensive repair and anesthesia of the entire extremity are often referred to a specialist, who may prefer to examine an unanesthetized limb. A nerve block is indicated when it will provide advantages over other techniques. Scenarios in which this requirement is met include the following: • When distortion from local infiltration hampers closure (e.g., facial wounds) or compromises blood flow (e.g., fingertip) • When anesthesia is required over a large area and multiple injections would be painful or when the large amount of anesthetic needed for local infiltration exceeds the recommended dose • When a nerve block is the most efficacious form of treatment, such as an intercostal block for treating a rib fracture or a patient with chronic obstructive pulmonary disease • When local infiltration of the wound would be more painful than a regional nerve block, such as in the plantar surface of the foot or the palm of the hand • When the block is performed to decrease pain during finger or toe dislocation or reduction • When extensive limb surgery or manipulation is required (e.g., extensive tendon repair) and other options are not available Factors influencing the choice of anesthetic agent for nerve blocks are similar to those for local infiltration (see Chapter 29 for extensive discussion). In general, most nerve blocks are done for the repair of painful traumatic injuries that are likely to cause pain long after the repair is completed. In such cases, select the anesthetic with the longest duration of action to maximize the patient’s analgesia. For most of the blocks described in this chapter, 0.25% bupivacaine is suggested as the anesthetic of choice, but equal volumes of 1% lidocaine with epinephrine can be substituted. The use of epinephrine on end-organ areas has traditionally been discouraged (e.g., tip of the nose, peripheral ear pinna, distal end of the penis), although the theoretical risk is unsubstantiated in clinical practice. Recent literature describes the use and confirms the safety of lidocaine with epinephrine (1 : 100,000 concentration) for digital blocks.1 It would be prudent to avoid epinephrine-containing anesthetics in injuries involving vascular compromise or for those with obvious peripheral artery disease. Higher concentrations of lidocaine (≤2%) or bupivacaine (0.5%) are commonly used for large nerves. Ropivacaine is a relatively new amide anesthetic with a rapid onset and a long duration of action (several hours). It has been reported to have fewer cardiotoxic and central nervous system effects than bupivacaine does.2,3 Take care to avoid exceeding the recommended dosages of the anesthetic chosen. Buffering the anesthetic is strongly encouraged to lessen the pain of infiltration (see Chapter 29). Use of ultrasound to identify injection sites for peripheral nerve blocks has been gaining popularity. Ultrasound guidance has been used successfully to locate and block nerves in the neck (e.g., interscalene and phrenic nerve blocks), lower extremity (e.g., femoral and saphenous nerve blocks), upper extremity (e.g., radial, ulnar, and median nerve blocks at the elbow), and the lumbar plexus.4–7 Ultrasonographic guidance negates the effects of anatomic variability, provides real-time needle guidance, and allows the operator to visualize the “spread” of local anesthetic. A common technique to ensure that the tip of the needle is in close proximity to the nerve is to elicit a paresthesia. Touching and mechanically stimulating the nerve with movement of the needle tip produces a tingling sensation or jolt known as a paresthesia, and it is felt along the distribution of the nerve. In practice, the jolt of a true paresthesia is often difficult to distinguish from the “ouch” of a pain-sensitive structure. When blocking proximal nerves at the elbow or axilla, the paresthesia travels far enough away from the injection site that it can be reliably distinguished from locally induced pain. Paresthesias at the level of the hand and wrist are more difficult to distinguish from pain. In both cases, paresthesia is a subjective feeling that requires intelligent and cooperative patients to understand what they are expected to feel and to remain relaxed and attentive so that they can distinguish an “ouch” from a jolt. Before the procedure, a simple explanation of what the patient should or may feel will facilitate cooperation. While eliciting paresthesias is generally reliable in demonstrating that the needle is close to its target, some authors believe that it may theoretically increase the rate of complications as a result of mechanical trauma or intraneural injection.8–10 Once the paresthesia is elicited, it is important to withdraw the needle 1 to 2 mm before injecting the anesthetic. If a paresthesia persists, stop the injection and reposition the needle. Nerve injury is rare but can occur secondary to (1) chemical irritation from the anesthetic, (2) direct trauma from the needle, or (3) ischemia as a result of intraneural injection. Overall, the incidence of serious neuronal injury is rare and occurs in 1.9 per 10,000 blocks.11 Given that placement of a nerve block is a blind procedure, nerve injuries do not necessarily represent an error in technique. Chemical neuritis from the anesthetic is the most common nerve injury.9,10 The patient may complain of pain and varying degrees of nerve dysfunction, including paresthesia or motor or sensory deficit. Most cases are transient and resolve completely. Supportive care and close follow-up are the mainstays of treatment. Emergency clinicians should not exceed the recommended doses and concentrations of anesthetic (Table 31-1). In general, lidocaine 1% or 2% or bupivacaine 0.25% or 0.5% is safe for nerve blocks performed in the ED. TABLE 31-1 Recommended Volumes of Anesthetic for Various Nerve Blocks *Anesthetic: 1% lidocaine or 0.25% bupivacaine (both with epinephrine). †Anesthetic: 1% lidocaine or 0.25% bupivacaine (both without epinephrine). Intraarterial injection of anesthetics with epinephrine may cause peripheral vasospasm and further compromise injured tissue. Intravascular anesthetic is not toxic to the limb itself, although it may produce transient blanching of the skin by displacing blood from the vascular tree. Epinephrine, however, can cause prolonged vasospasm and subsequent ischemia if it is injected into an artery. This is especially worrisome when anesthetizing areas with little collateral circulation, such as the toes, fingers, penis, and tip of the nose. Severe epinephrine-induced tissue blanching or vasospasm may be reversed with local or intravascular injection of phentolamine (see extensive discussion in Chapter 29). Vasospasm associated with the epinephrine in anesthetic solutions is rare, but experience in related clinical situations can help guide therapy. Roberts and Krisanda used a total of 5 mg of phentolamine infused intraarterially to reverse arm ischemia following 3 mg of epinephrine inadvertently administered into the brachial artery during cardiac resuscitation.12 Digital ischemia from inadvertent epinephrine autoinjection (Epi-Pen) has been treated both by proximal “digital block” with 2 mg of phentolamine and by local infiltration at the ischemic site with 1.5 mg of phentolamine.13,14 The route of phentolamine administration should be guided by the clinical situation. Phentolamine must reach the site of vasospasm. Local infiltration may be effective for ischemia in a single toe or finger, whereas arterial injection has the advantage of delivering the medication directly to the arteries exhibiting spasm. For larger areas of involvement or in instances in which local infiltration is ineffective, use intraarterial injection. A dose of 1.5 to 5 mg appears to be effective in most cases,12–14 although a total of 10 mg may be used for local infiltration. Phentolamine, 5 mg, can be mixed with 5 to 10 mL of either normal saline or lidocaine. The small volume of the distal pulp space may limit the volume of the infiltration dose to 0.5 to 1.5 mL in the fingertip. Larger volumes and dosages can be used with proximal infiltrations. For intraarterial infusion of the radial artery at the wrist or the dorsalis pedis at the ankle, dosages of 1.5 to 5 mg of phentolamine are suitable. Slow infusion or graded dosages of 1 mg may provide enough phentolamine to reverse the ischemia without excessive systemic effects such as hypotension. The incidence of systemic toxicity with local anesthetics has diminished significantly in the past 30 years. Interestingly, peripheral nerve blocks have been reported to have the highest incidence of systemic toxicity.11 Allergic reactions account for only 1% of untoward reactions (see Chapter 29).15 Blocking the intercostal nerves produces anesthesia over an area of their cutaneous distribution (Fig. 31-1) and provides considerable pain relief for patients with rib contusions or fractures. Rib fractures are typically quite painful and cause the patient to try to splint respirations to avoid excessive movement of the injured site. The resulting hypoventilation, atelectasis, and poor expectoration from splinting respirations may cause hypoxia or lead to pneumonia. This is particularly true in patients with preexisting pulmonary disease and minimal respiratory reserve, in whom further impairment of function may cause significant respiratory compromise. Figure 31-1 A and B, Intercostal nerve block: area of anesthesia and cutaneous distribution of the intercostal nerves. Theoretically, anesthetizing injured ribs eases pain and facilitates deep breathing and coughing. Unfortunately, no controlled studies have compared intercostal blocks and oral analgesics in patients with the types of rib fractures that are commonly managed on an outpatient basis. However, studies do suggest that intercostal blocks may be superior to analgesics in patients who have undergone thoracotomy.16–18 In these studies, those receiving intercostal nerve blocks had better results on pulmonary function tests, greater oxygenation, and earlier ambulation and discharge than did those receiving opioid analgesics. Finally, a wrongly perceived high incidence of pneumothorax and unsuccessful blocks deters many clinicians from performing intercostal nerve blocks in the ED. The true incidence of pneumothorax after intercostal nerve blocks is very low and not significant enough to prohibit the procedure. Moore reported that in more than 10,000 individual rib blocks performed, the incidence of pneumothorax was less than 0.1%.19 However, Shanti and associates reported that the incidence of pneumothorax was 1.4% for each individual intercostal nerve blocked.20 If more than one nerve requires blockade, the incidence of pneumothorax may be greater. The suggested approach to discussing intercostal blocks is to give patients the facts with regard to the duration of analgesia and possible complications and then allow them to decide on the method for themselves. Frequently, they prefer oral analgesics initially but may return for further relief of pain, at which time they are more amenable to a nerve block. Each thoracic nerve exits the spine through the intervertebral foramen, which lies midway between adjacent ribs (Fig. 31-2A). It immediately gives off the posterior cutaneous branch, which supplies the skin and muscles of the paraspinal area. The intercostal nerve then continues around the chest wall and gives off lateral cutaneous branches at the midaxillary line. These branches are the sensory supply to the anterior and posterior lateral chest wall. To achieve adequate analgesia for most rib fractures, the lateral cutaneous branch needs to be anesthetized. Therefore, perform blocks between the posterior axillary and midaxillary line at a point proximal to the origin of this branch (see Fig. 31-2A, arrow). Explain the procedure and its benefits and its risks, including potential pneumothorax, systemic toxicity, and ineffective block, before proceeding. Use a 10-mL syringe with a 3.75-cm, 25-gauge needle. Prepare the area to be injected in the usual aseptic manner. Use the index finger of the nondominant hand to retract the skin at the lower edge of the rib cephalad and pull it up and over the rib (see Fig. 31-2B). With the syringe in the opposite hand, puncture the skin close to the tip of the finger that is retracting the skin over the rib. Keep the syringe at an 80-degree angle to the chest wall with the needle pointing cephalad, and rest the hand holding the syringe on the chest wall for stability. In this position, the depth of needle penetration is well controlled. Slowly advance the needle until it comes to rest on the lower border of the rib. The bone should be felt through the tip of the needle. If the clinician inadvertently causes a pneumothorax, treatment depends on its size. Many pneumothoraces from this procedure are small and require no specific intervention. Those smaller than 20% may be observed for 6 hours.21 During this time, administer a high concentration of oxygen to help decrease the size of the pneumothorax. If the pneumothorax does not enlarge, the patient may be released home with arrangements for close follow-up. Needle or catheter aspiration of larger pneumothoraces may be all that is needed. A chest tube is necessary if this method fails (see Chapter 10). The median, ulnar, and radial nerves can be blocked at the elbow to provide anesthesia to the distal end of the forearm and hand (Fig. 31-3). For most injuries extensive enough to require a nerve block at the elbow, all three nerves must be blocked for successful anesthesia because of the variable and overlapping innervation of the forearm. Furthermore, injuries to the proximal and middle aspects of the forearm may require additional circumferential subcutaneous field blocks of the lateral, medial, and posterior cutaneous nerves. Ulnar Nerve: Anatomy and Technique (Fig. 31-4A): The ulnar nerve can be palpated in the ulnar groove on the posteromedial aspect of the elbow between the olecranon and the medial condyle of the humerus. This nerve supplies innervation to the small finger, the ulnar half of the ring finger, and the ulnar aspect of the hand.
Nerve Blocks of the Thorax and Extremities
General Concepts
Preparation
Choice of Anesthetic
Locating the Nerve
Ultrasound
Paresthesia
Complications and Precautions
Nerve Injury
Intravascular Injection
Systemic Toxicity
Specific Nerve Blocks
Anatomy
Technique
Precautions
Nerve Blocks of the Upper Extremity
Nerve Blocks at the Elbow
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Nerve Blocks of the Thorax and Extremities