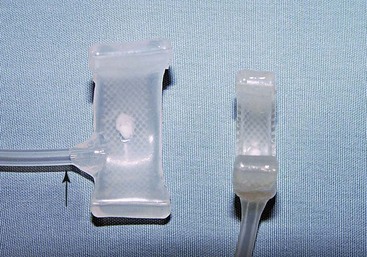
Chapter 202 Pharmacologic therapy is the standard of care for initial treatment of dogs with acquired urinary incontinence. Although treatment with α-agonists or estrogenic compounds (see Chapter 201) is effective in the majority of animals with acquired urinary incontinence, in approximately 20% of dogs with USMI the disorder is refractory to medical therapy. Male dogs with USMI and dogs with congenital malformations are far less likely to respond to drug therapy. Endoscopic or surgical procedures are considered as a means to improve control of urinary incontinence when the disorder shows no response to medical therapy or when clients feel that the lifelong administration of drugs is undesirable. Historically, endoscopic application of urethral bulking agents has provided a minimally invasive method for the treatment of USMI in female dogs (see Web Chapter 71). Although this procedure is effective in the majority of dogs (66% rate of complete continence; Byron et al, 2011), the durability of this effect is poor, with the mean duration of continence ranging from 5.2 to 16.4 months. In addition, the length of the male canine urethra makes endoscopic urethral bulking techniques impractical for use in male dogs. Because of the need for repeated injections over time and the limited availability of suitable bulking agents, many referral practices are actively seeking out other means of therapy for refractory incontinence. The canine artificial urethral sphincter (AUS; Figure 202-1) is a modification of an inflatable silicone hydraulic vascular occluder that was intended for use in the temporary constriction of blood vessels in laboratory animals (Adin et al, 2004; Sereda et al, 2005). The device is similar in concept to an artificial urethral sphincter used in human beings with urinary incontinence (AMS 800), although that device requires manual deflation before each act of urination—a feature that prevented its direct application in dogs. Instead, the canine AUS is designed to produce a low level of static urethral compression, similar to the effect of urethral bulking agents. After the device was evaluated in cadavers, it was determined that these inflatable cuffs could be placed around the canine urethra through a caudal abdominal approach. Actuating tubing from the cuff is connected to a permanent subcutaneous injection port (Le Grande CompanionPort vascular access port) that is placed under the skin on the caudoventral abdomen. Incremental injections of fluid into the port created corresponding increases in urethral pressure in the cadaver study (Adin et al, 2004). Mechanical studies showed that devices that were inflated with sterile 0.9% NaCl remained inflated over a 5-month period of immersion in simulated body fluid (Sereda et al, 2006). Based on the success of these initial investigations and a subsequent pilot study in four client-owned dogs with refractory USMI (Rose et al, 2009), we now have performed the procedure in over 30 dogs with an expanding list of acquired and congenital causes of urinary incontinence. Figure 202-1 The silicone canine artificial urethral sphincter (AUS; DocXS Biomedical Products) at the left is a modification of a hydraulic vascular occluder (right). The AUS cuff was widened to 1.4 cm to minimize atrophy of the urethra at an area of focal compression. The actuating tube (arrow), used to inflate the device by injections into a subcutaneous port, was changed to a side-entry design to prevent kinking of the device on the urethra when the device is placed in the pelvic canal.
Mechanical Occluder Devices for Urinary Incontinence
Therapeutic Options
Artificial Urethral Sphincter
< div class='tao-gold-member'>
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


