CHAPTER 76 Management of Tongue Injuries
The horse’s tongue is a highly mobile, muscular organ that is covered with a tough, specialized squamous epithelium modified to form papillae. By virtue of its relative degree of exposure to the environment, the rostral spatulated portion of the tongue is susceptible to injury. Traumatic injury can arise from bits or other tack placed in the oral cavity, from sharp external objects, blows to the head, injury during recovery from general anesthesia, and iatrogenic damage during intraoral procedures such as dental extraction or transoral epiglottic entrapment release. Injury from a penetrating foreign body, typically wire, is not uncommon, and neurogenic injury is possible.
TRAUMATIC INJURIES
Severe Deep Lacerations
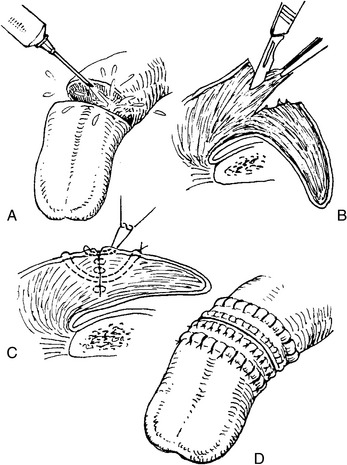
Primary closure of severe tongue lacerations is encouraged when possible. The wound edges are debrided of necrotic and contaminated tissue and lavaged vigorously. A multilayer closure to eliminate dead space is recommended. To relieve tension on the closure, vertical mattress sutures are preplaced deep in the muscular body of the tongue with absorbable or nonabsorbable, size 0 or 1, monofilament suture. Buried rows of simple interrupted monofilament absorbable sutures of size 2-0 to 0 are placed to appose the muscles and obliterate dead space. The vertical mattress sutures are tied, and the lingual mucosa is apposed with simple continuous or interrupted vertical mattress sutures of size 2-0 or 0 absorbable suture (Figure 76-1).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


